Download
1 / 37
410 likes | 757 Views
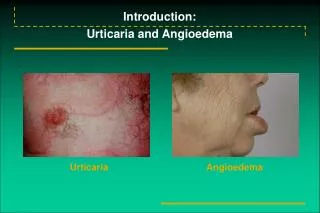
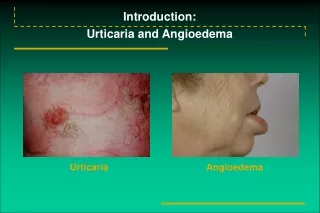
Angioedema 11/12/2010. BY: MOHAMMED ALSAIDAN. Angioedema. Abrupt and short-lived swelling of the skin, mucous membranes, or both including the upper respiratory and intestinal epithelial linings The swelling is nonpitting, erythematous or skin-colored Areas where the skin is lax

E N D
Angioedema11/12/2010 BY: MOHAMMED ALSAIDAN
Angioedema • Abrupt and short-lived swelling of the skin, mucous membranes, or both including the upper respiratory and intestinal epithelial linings • The swelling is nonpitting, erythematous or skin-colored • Areas where the skin is lax • Pain is variable, but rarely itching. • There is no desquamation or staining of the skin although scratching or rubbing may cause bruising.
Pathophysiology • Increase in permeability of the submucosal or subcutaneous capillaries and postcapillary venules, causing local plasma extravasation and consequent swelling. • A variety of vasoactive molecular mediators , by mast cells: • Preformed ? synthesized ? • There is a paucity of cellular infiltration in angioedema.
Epidemiology • 49% of all patients with urticaria also had angioedema • Angioedema occurred in 93 of 107 (87%) patients with chronic urticaria • Women are more frequently affected than men • Most commonly affects those 40 to 50 years old
Acute allergic angioedema • Almost always accompanied by urticaria , within 1 to 2 hours of exposure to the offending allergen. • It is commoner in patients who are atopic or allergic to foods or medications • Pathophysiology = urticaria • (the g-chains of FceR1 tyrosine kinase activation protein kinase C activation increase in intracellular calcium mast cell degranulation )
Acute allergic angioedema • Clinical features: swelling can occur anywhere • Risk of anaphylaxis • Skin prick test vs. RAST
TREATMET • ABC • EPI PEN Adult Mild angioedema without signs of circulatory compromise 0.3-0.5 mg of 1:1000 SC Moderate-to-severe angioedema with signs of shock: Adult dose is 0.3-0.5 mg of 1:10,000 IV Pediatric0.15-0.3 mg (depending on the patient's weight) of 1:1000 solution SC • Diphenhydramine (50 mg) I.V. or I.M • Hydrocortisone (200 mg) I.V • 24 h. Observation
NSAID-induced angioedema • Clinical picture resemble allergic urticaria or angioedema and are often termed ‘‘pseudoallergic” • Only COX 1 inhibitors cause pseudoallergic angioedema • Skin prick testing has no value • urticaria/angioedema to NSAIDS vs. NSAID-induced asthma • Rx: Emergency measures are as for acute allergic angioedema +/- leukotriene antagonists?
Angioedema of ACE inh. • Not associated with urticaria • Usually involve face + orophaynx • Incidence = 0.1% to 0.2% and is 5 x more common in African Americans than white patients • The most common cause of acute angioedema • Rx: as for allergic but with risk of relapses after recovery
Angioedema of ACE inh. • Angiotensin II receptor antagonists are tolerated by patients who have reacted to ACE inhibitors • Screen for HAE
Idiopathic acquired angioedema • Chronic and relapsing, and usually associated with urticaria • In 30% to 50% : urticaria and the angioedematous lesions are a result of an autoimmune process • Angioedema and urticaria occurred together in 49% to 87% and angioedema alone in 9 to 11% • Pathophysiology = idiopathic urticaria • ASST might be helpful, basopenia
Idiopathic acquired angioedema • Avoid provoking factors : • Aspirin • Overtiredness • Overexcitement • overvigorous exercise • alcohol overconsumption • Antihistamines vs. steroids vs. others?
Gleich syndrome • Episodic angioedema, urticaria, fever, weight gain, peripheral blood and skin eosinophilia • Patients responded well to systemic steroids • Probably closely related to the hypereosinophilic syndrome
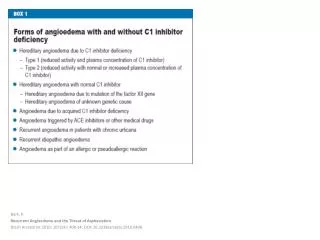
Hereditary angioedema (HAE) • Dominantly inherited defect in chromosome 11 (11q12-q13.1) • Affects about 1:50,000 person • (type 1) (The classic type) is a quantitative defect in (C1 INH) • (type 2) is functional defect in (C1 INH) • (type 3) in women with quantitatively and functionally normal C1 INH activity with a relationship to estrogenic activity
To be clinically expressed , the C1 INH plasma level should be quantitatively or functionally less than 40% of normal
Hereditary angioedema (HAE) • Increase in activation of C1, leading to consumption of C2 and C4, high level of bradykinin • Patients are usually asymptomatic up to puberty • precipating factors • minor injury such as dental maneuvers (>50%) • vigorous exercise • alcohol consumption • emotional stress • hormonal factors
Hereditary angioedema (HAE) • There could be transitory prodromalnonpruriticurticarial eruption in some patients, persist for 3 to 4 days • Coadministration of ACE inhibitors and estrogens is contraindicated in HAE. • Associated diseases: • Glomerulonephritis • Sjogren’s syndrome • thyroiditis, • Lupus • coagulopathies
Treatment • ABCs (usually not life threatening) • Antihistamines and corticosteroids are ineffective • S.C. adrenaline (0.3 mg every 10 minutes) usually not effective but maybe helpful • The mainstay treatment is: I.V. FFP or C1 inhibitor concentrate • 550 plasma U in a 10-mL vial to be administered at a dose of 25 plasma U/kg body weight to a total of 1000 plasma U repeated once if necessary, It is usually effective within 3 to 4 hours, and often within minutes.
Treatment • There have been reports of improvement of acute symptoms with icatibant, a specific B2 kinin antagonist • Anabolic steroids • increase the circulating levels of normal functional C1 INH in both type 1 and type 2 HAE • risk of hepatotoxicity and liver adenomas • stanazolol 2-4 mg/d • danazol 50-300 mg/d • women : hirsutism, acne, menstrual cycle irrigularity, deep voice
Prophylaxis • C1 inh concentrate before surgery, especially when intubation or tooth extraction is necessary • For minor surgical procedures, tranexamic acid (1 g four times daily in adults or 500 mg four times daily in children) for 48 hours before and after the procedure • increase in established maintenance doses of tranexamic acid or anabolic steroids
Acquired C1 inh. deficiency • Type 1: immune complex mediated C1 and C1 inh consumption • associated diseases : • B-cell lymphoma (the most common) • Other haematologic malignancies • Type 2 : autoantibodies against C1 inh.
Treatment • Treatment of the underlying disease • Plasma or C1 inhibitor concentrate used for emergency • For chronic disease: • Plasmapheresis • Cytotoxic agent • Androgenic compounds • e-aminocaproic acid • Tranexamic acid for type II