Download
1 / 44
580 likes | 1.46k Views
Chronic Kidney Disease/Dialysis. Belinda Jim, MD January 15, 2009. Definition. NKF’s (National Kidney Foundation’s) K/DOQI (Kidney Disease Outcomes Quality Initiative) Work Group criteria for CKD are: Kidney damage for >3months, with or without decreased GFR manifest by either:

E N D
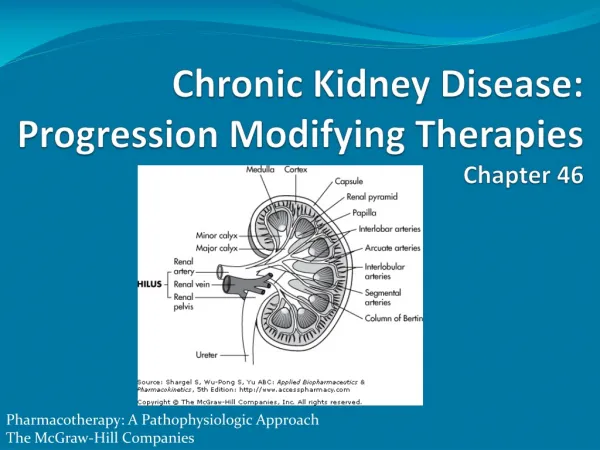
Chronic Kidney Disease/Dialysis Belinda Jim, MD January 15, 2009
Definition • NKF’s (National Kidney Foundation’s) K/DOQI (Kidney Disease Outcomes Quality Initiative) Work Group criteria for CKD are: • Kidney damage for >3months, with or without decreased GFR manifest by either: • Pathological abnormalities or • Markers of kidney damage, including abnormalities in the composition of the blood or urine, or abnormalities in the imaging tests. OR • GFR < 60ml/min/1.73m2 for >3months
Causes of ESRD • Regardless of acute or chronic, should calculate renal function by eGFR • Used to evaluate extent of impairment, follow course of disease and response to therapy • Dose adjustments
Equations to Estimate GFR • Gold Standard – inulin clearance, I-iothalmate, Tc-DTPA clearance. These tests are not uniform. • Cockcroft-Gault equation- • (140-age) x wt/ 72 x SCr. (x 0.85 for women). • MDRD (Modification of Diet in Renal Disease) – Abbreviated version • 186 x SCr. To power of -0.203 (x 0.742 if female) and (x1.210 if black). • 24 hr. Urine for Cr.Cl – • GFR = UCr.V/PCr x 0.70 (to convert to ml/min)
CKD Staging and Prevalence Coresh et al , J Am Soc Nephrol, 2005; 16: 180-188Data supplied by USRDS 2004 Annual Data Report.
Natural History of Renal Disease • Initial injury may vary in pathogenesis • Kidney adapts by increasing filtration rate in remaining normal nephronsadaptive hyperfiltration • Long-term damage, manifested by proteinuria and progressive renal insufficiency • Gradual decline usually asymptomatic • No exact correlation between level of BUN and symptoms • Uremic symptoms: anorexia, nausea, vomiting, fatigue, hiccups, pruritis
General Management • Treatment of reversible causes • Decreased renal perfusion • Administration of nephrotoxic drugs • Urinary tract obstruction • Prevention or slow the progression • Treatment of complications • Identification and adequate preparation of renal replacement therapy (RRT)
Factors Affecting Progression of CKD Non-Modifiable Risk Factors: • Age – incidence climbs after 65 • Gender – more common in males with a faster rate of decline. • Race – incidence higher in AA and Hispanics. • Genetics – diabetic and non-diabetic nephropathies cluster in families.
Modifiable Risk Factors • Proteinuria – aim for <500mg/24hr. • Hypertension – aim for <130/80 or MAP <90 with ACE I/ARB. • Glycemic control – Evidence is conflicting in progression of CKD. • Dyslipidemia – elevated levels associated with more rapid decline – esp in DN. • Obesity - linked to faster rate of progression in CKD. • Hyperuricemia – May cause renal injury and HTN through stimulationof renin-angiotensin system.
Treatment of Complications • Volume overload • Hyperkalemia • Metabolic acidosis • Hyperphosphatemia • Anemia • Hyperparathyroidism • Bone disease • Uremic symptoms
Volume Overload • Sodium and intravascular volume balance usually maintained until GFR falls below 10 to 15 ml/min • Mild to moderate CKD less able to respond to rapid infusions of sodium, prone to overload • Respond to combination of dietary sodium restriction and diuretic therapy
Hyperkalemia • Problem with • Aldosterone • Distal flow in kidney (eGFR<10 -15ml/min). • Patient is either: • Oliguric. • Has high K diet. • Has increased tissue breakdown. • Has Hypoaldosteronism (eg. ACE Inhibitors, type IV RTA). • Treatment consists of low K diet (2gm/day), diuretics and kayexalate.
Metabolic Acidosis • Increasing tendency to retain H+ • Decreased HCO3-, usually between 12-20meq/L • Bone buffering of excess H+ ions associated with release of Ca2+ and Phos from bone • Uremic acidosis increase skeletal muscle breakdown and diminish albumin synthesis loss of lean muscle mass and fatigue • Sodium bicarbonate or sodium citrate to keep HCO3 above 22meq/L
Treatment of Secondary Hyperparathyroidism • Phosphate binders: • Low Phos diet (<800 mg/day) • Ca based: • CaCO3 • Ca acetate • Non absorbable agent: • Sevelamer Hydrochloride (Renagel) • Sevelamer Carbonate (Renvela) • Lanthanum carbonate (Fosrenol) • Aluminum binders. • Vitamin D analogs: • Calcitriol (Rocaltrol) • Paricalcitol (Zemplar) • Doxercalciferol (Hectoral) • Calcimimetic: Cinacalcet (Sensipar)
Renal Osteodystrophy • Types of Bone Disease • Osteitis fibrosa • Osteomalacia • Adynamic bone disease • Target PTH • Stage 3 (GFR 30-59): 35-70 pg/mL • Stage 4 (GFR 15 to 29): 70-110 pg/mL • Stage 5 (GFR less than 15): 150-300 pg/mL
Hypertension • Mostly volume mediated • Start with ACEI/ARB and diuretic • Thiazides become ineffective when GFR falls below 20 • Goal is less than 130/80, but even lower systolic with urine prot/creat >1
Anemia in CKD • The primary cause of anemia in patients with CKD is insufficient production of erythropoietin (EPO) by the diseased kidneys. • Other causes include: • Iron deficiency. • Secondary hyperparathyroidism. • Decreased RBC lifespan. • Folate deficiency.
K/DOQI Guidelines for Anemia in CKD • Target Hgb between 11-12 g/dL • Anemia work-up when • Hgb <11g/dL (Hct is <33 percent) in pre-menopausal females and pre-pubertal patients. • Hgb <12g/dL (Hct is <37 percent) in adult males and post-menopausal females. • Use of erythropoietic agents (Epo,Procrit,Aranesp)
Dyslipidemia • Primary finding in CKD is hypertriglyceridemia • Goal of LDL in CKD in similar to CHD – LDL <100, but there is not much evidence whether this is beneficial. • One large study in CKD Stage V showed a negative association with very low cholesterol levels
Preparation for Renal Replacement Therapy • Refer to nephrology when GFR < 60 • Early education of CKD • Choice of renal replacement therapy • In-center hemodialysis • Peritoneal dialysis • Home hemodialysis • Access placement • Referral to vascular surgery of AVF placement if patient choses HD and advising patient to save non-dominant arm from venopuctures and heplocks.
Initiation of Emergent Dialysis • Uremic syndrome • Refractory volume overload • Uncontrollable hyperkalemia • Severe metabolic acidosis • Steady worsening of renal function, with BUN exceeding 70-100 mg/dL or creatinine clearance of less than 15-20 ml/min/1.73 m2
Diffusion • Transport process by which a solute passively diffuses down its concentration gradient from one fluid compartment into the other
Ultrafiltration (UF) • Fluid removal occurs via hydrostatic pressure gradient across membrane generated by dialysis machine
Peritoneal Dialysis (PD) • Uses peritoneal membrane to transport solutes and water across two compartments • One compartment is blood in the peritoneal capillaries, second compartment is dialysate solution in peritoneal cavity
Continuous Renal Replacement Therapies (CRRTs) • Slower rate of solute or fluid removal per unit of time • Slower blood flow rate for the hemodynamically unstable patient • Better tolerated than conventional therapy
Complications • Hypotension • Infection • Catheter Dysfunction
Hypotension • Common Causes Fluctuations in UF rate High UF rate Target dry weight set too low Dialysis solution too warm Food ingestion Autonomic neuropathy Antihypertensive medications
Hypotension-Cardiac • Diastolic dysfunction due to LVH, ischemic heart disease • Failure to increase cardiac rate • Inability to increase cardiac output for other reasons
Hypotension • Less common reasons • Pericardial tamponade • Myocardial infarction • Arrhythmia • Occult hemorrhage • Dialyzer reaction • Hemolysis • Air embolism
Dialysis Catheter Infections • Localized exit site infection • Erythema and/or crust, no purulent discharge, treat with antibiotics for up to 2 weeks • Tunnel Infection • Purulent exudate present, and pain/warmth along the tunnel, removal of catheter with antibiotic administration for 3 weeks • Systemic Infection • Fever, leukocytosis, may have no overt signs of catheter infection
Microbiology • Staph species (40-81%) • Enterococci, gram neg organisms, fungal organisms • Empiric treatment with Vancomycin and Gentamicin • Treat with Nafcillin if MSSA!
Complications of Catheter Infection • Endocarditis • Osteomyelitis • Thrombophlebitis • Spinal epidural abscess
Catheter Dysfunction • Early • less than 5 days • Due to malposition or to intracatheter thrombosis • Fibrin sleeves and mural thrombi • Treatment • Catheter exchange • TPA
Catheter Dysfunction • Late (more than 5 days) • More likely due to intracatheter thrombosis than malposition • Treatment • TPA • Catheter exchange
Vascular Access • Permanent catheter • AV graft • AV fistula
Permanent Catheter • Cuffed venous catheters an alternative form of long-term access • High rate of complications • Thrombosis • Infection • Inadequate blood flow
AV Graft Advantages • AV connection made using a tube graft from synthetic material • Maturation requires 2-3 weeks for adhesion of subcutaneous tunnel and graft Disadvantages • Higher rates of infection • Higher rates of thrombosis • Shorter lifespan
AV fistula Advantages • Subcutaneous anastomosis of artery to adjacent vein • Safest longest lasting permanent access • Excellent patency • Lower morbidity • Lower complication Disadvantages • Long maturation time • Failure to mature in some patients • May not be feasible in patients with vascular disease