Download
1 / 1
10 likes | 250 Views
Maternal and Neonatal Outcomes in Pregnancies Complicated by Antepartum Hemorrhage and Hospital Admission. 3819 women entered into CPN. 969 (25.4%) admitted with APH. 806 women followed to delivery. 163 lost to follow-up. 784 women with baby information.

E N D
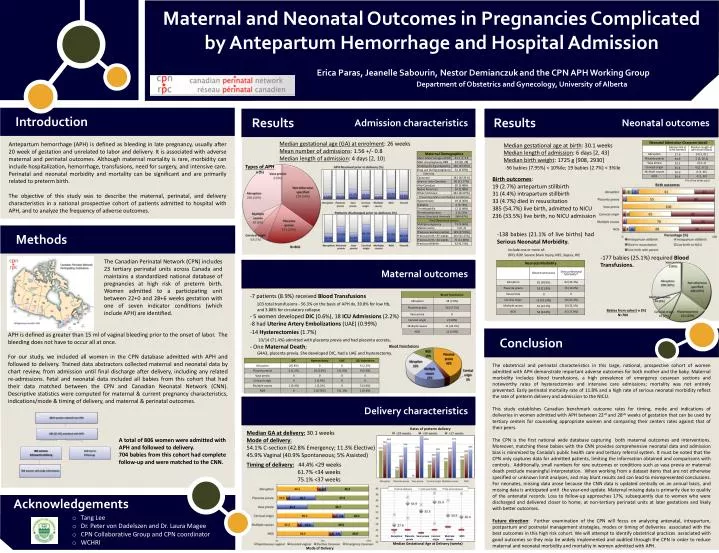
Maternal and Neonatal Outcomes in Pregnancies Complicated by Antepartum Hemorrhage and Hospital Admission 3819 women entered into CPN 969 (25.4%) admitted with APH 806 women followed to delivery 163 lost to follow-up 784 women with baby information Erica Paras, Jeanelle Sabourin, Nestor Demianczukand the CPN APH Working Group Department of Obstetrics and Gynecology, University of Alberta Results Results Admission characteristics Neonatal outcomes Introduction Median gestational age (GA) at enrolment: 26 weeks Mean number of admissions: 1.56 +/- 0.8 Median length of admission: 4 days [2, 10] Antepartum hemorrhage (APH) is defined as bleeding in late pregnancy, usually after 20 week of gestation and unrelated to labor and delivery. It is associated with adverse maternal and perinatal outcomes. Although maternal mortality is rare, morbidity can include hospitalization, hemorrhage, transfusions, need for surgery, and intensive care. Perinatal and neonatal morbidity and mortality can be significant and are primarily related to preterm birth. The objective of this study was to describe the maternal, perinatal, and delivery characteristics in a national prospective cohort of patients admitted to hospital with APH, and to analyze the frequency of adverse outcomes. Median gestational age at birth: 30.1 weeks Median length of admission: 6 days [2, 43] Median birth weight: 1725 g [908, 2930] -56 babies (7.95%) < 10%ile; 19 babies (2.7%) < 3%ile Birth outcomes: 19 (2.7%) antepartum stillbirth 31 (4.4%) intrapartum stillbirth 33 (4.7%) died in resuscitation 385 (54.7%) live birth, admitted to NICU 236 (33.5%) live birth, no NICU admission Types of APH n (%) Birth outcomes (*% of live-births only) -138 babies (21.1% of live births) had Serious Neonatal Morbidity. Include one or more of: BPD, ROP, Severe Brain Injury, NEC, Sepsis, HIE N=806 -177 babies (25.1%) required Blood Transfusions. Maternal outcomes Methods The Canadian Perinatal Network (CPN) includes 23 tertiary perinatal units across Canada and maintains a standardized national database of pregnancies at high risk of preterm birth. Women admitted to a participating unit between 22+0 and 28+6 weeks gestation with one of seven indicator conditions (which include APH) are identified. -7 patients (8.9%) received Blood Transfusions 103 total transfusions - 56.3% on the basis of APH dx, 39.8% for low Hb, and 3.88% for circulatory collapse - 5 women developed DIC (0.6%), 18 ICU Admissions (2.2%) -8 had Uterine Artery Embolizations (UAE) (0.99%) 6/8 required hysterectomies -14 patients required Hysterectomies; 10/14 (71.4%) were admitted with bleeding from placenta - Babies from cohort n (%) N=704 • 14 Hysterectomies (1.7%) • 10/14 (71.4%) admitted with placenta previa and had placenta accreta. • - One Maternal Death; • G4A3, placenta previa. She developed DIC, had a UAE and hysterectomy. APH is defined as greater than 15 ml of vaginal bleeding prior to the onset of labor. The bleeding does not have to occur all at once. For our study, we included all women in the CPN database admitted with APH and followed to delivery. Trained data abstractors collected maternal and neonatal data by chart review, from admission until final discharge after delivery, including any related re-admissions. Fetal and neonatal data included all babies from this cohort that had their data matched between the CPN and Canadian Neonatal Network (CNN). Descriptive statistics were computed for maternal & current pregnancy characteristics, indications/mode & timing of delivery, and maternal & perinatal outcomes. Conclusion Blood Transfusions The obstetrical and perinatal characteristics in this large, national, prospective cohort of women admitted with APH demonstrate important adverse outcomes for both mother and the baby. Maternal morbidity includes blood transfusions, a high prevalence of emergency cesarean sections and noteworthy rates of hysterectomies and intensive care admissions; mortality was not entirely prevented. Early perinatal mortality rate of 11.8% and a high rate of serious neonatal morbidity reflect the rate of preterm delivery and admission to the NICU. This study establishes Canadian benchmark outcome rates for timing, mode and indications of deliveries in women admitted with APH between 22+0 and 28+6 weeks of gestation that can be used by tertiary centers for counseling appropriate women and comparing their centers rates against that of their peers. The CPN is the first national wide database capturing both maternal outcomes and interventions. Moreover, matching these babies with the CNN provides comprehensive neonatal data and admission bias is minimized by Canada’s public health care and tertiary referral system. It must be noted that the CPN only captures data for admitted patients, limiting the information obtained and comparisons with controls. Additionally, small numbers for rare outcomes or conditions such as vasa previa or maternal death preclude meaningful interpretation. When working from a dataset items that are not otherwise specified or unknown limit analyses, and may blunt results and can lead to misrepresented conclusions. For neonates, missing data arose because the CNN data is updated centrally on an annual basis, and missing data is anticipated until the year-end update. Maternal missing data is primarily due to quality of the antenatal records. Loss to follow-up approaches 17%, subsequently due to women who were discharged and delivered closer to home, at non-tertiary perinatal units at later gestations and likely with better outcomes. Future direction: Further examination of the CPN will focus on analyzing antenatal, intrapartum, postpartum and postnatal management strategies, modes or timing of deliveries associated with the best outcomes in this high risk cohort. We will attempt to identify obstetrical practices associated with good outcomes so they may be widely implemented and audited through the CPN in order to reduce maternal and neonatal morbidity and mortality in women admitted with APH. Delivery characteristics Rates of preterm delivery Median GA at delivery:30.1 weeks Mode of delivery: 54.1% C-section (42.8% Emergency; 11.3% Elective) 45.9% Vaginal (40.9% Spontaneous; 5% Assisted) Timing of delivery: 44.4% <29 weeks 61.7% <34 weeks 75.1% <37 weeks A total of 806 women were admitted with APH and followed to delivery. 704 babies from this cohort had complete follow-up and were matched to the CNN. Acknowledgements • Tang Lee • Dr. Peter von Dadelszen and Dr. Laura Magee • CPN Collaborative Group and CPN coordinator • WCHRI Mode of Delivery Median Gestational Age at Delivery (weeks) Abruption Vasa previa NOS Placenta previa Cervical origin Multiple causes