Download
1 / 1
10 likes | 113 Views
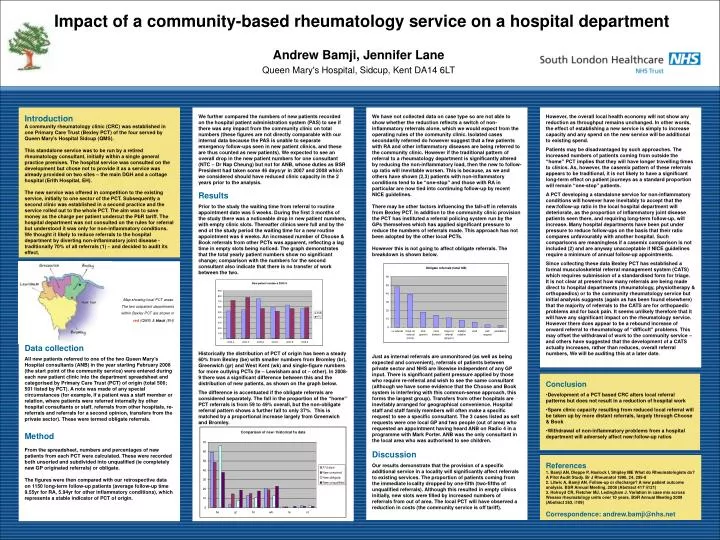
Impact of a community-based rheumatology service on a hospital department. Andrew Bamji, Jennifer Lane Queen Mary's Hospital, Sidcup, Kent DA14 6LT. Introduction

E N D
Impact of a community-based rheumatology service on a hospital department Andrew Bamji, Jennifer Lane Queen Mary's Hospital, Sidcup, Kent DA14 6LT Introduction A community rheumatology clinic (CRC) was established in one Primary Care Trust (Bexley PCT) of the four served by Queen Mary's Hospital Sidcup (QMS). This standalone service was to be run by a retired rheumatology consultant, initially within a single general practice premises. The hospital service was consulted on the development but chose not to provide it as a service was already provided on two sites – the main DGH and a cottage hospital (Erith Hospital, EH). The new service was offered in competition to the existing service, initially to one sector of the PCT. Subsequently a second clinic was established in a second practice and the service rolled out to the whole PCT. The aim was to save money as the charge per patient undercut the PbR tariff. The hospital department was not consulted on the rules for referral but understood it was only for non-inflammatory conditions. We thought it likely to reduce referrals to the hospital department by diverting non-inflammatory joint disease - traditionally 70% of all referrals (1) – and decided to audit its effect. We further compared the numbers of new patients recorded on the hospital patient administration system (PAS) to see if there was any impact from the community clinic on total numbers (these figures are not directly comparable with our internal data because the PAS is unable to separate emergency follow-ups seen in new patient clinics, and these are thus counted as new patients). We expected to see an overall drop in the new patient numbers for one consultant (NTC – Dr Nap Cheung) but not for ANB, whose duties as BSR President had taken some 46 days/yr in 2007 and 2008 which we considered should have reduced clinic capacity in the 2 years prior to the analysis. Results Prior to the study the waiting time from referral to routine appointment date was 5 weeks. During the first 3 months of the study there was a noticeable drop in new patient numbers, with empty clinic slots. Thereafter clinics were full and by the end of the study period the waiting time for a new routine appointment was 6 weeks. An increased number of Choose & Book referrals from other PCTs was apparent, reflecting a lag time in empty slots being noticed. The graph demonstrates that the total yearly patient numbers show no significant change; comparison with the numbers for the second consultant also indicate that there is no transfer of work between the two. Historically the distribution of PCT of origin has been a steady 60% from Bexley (be) with smaller numbers from Bromley (br), Greenwich (gr) and West Kent (wk) and single-figure numbers for more outlying PCTs (le – Lewisham and ot – other). In 2008-9 there was a significant difference between this and the distribution of new patients, as shown on the graph below. The difference is accentuated if the obligate referrals are considered separately. The fall in the proportion of the “home” PCT referrals is from 59 to 49% overall, but the non-obligate referral pattern shows a further fall to only 37%. This is matched by a proportional increase largely from Greenwich and Bromley. We have not collected data on case type so are not able to show whether the reduction reflects a switch of non-inflammatory referrals alone, which we would expect from the operating rules of the community clinic. Isolated cases secondarily referred do however suggest that a few patients with RA and other inflammatory diseases are being referred to the community clinic. However if the traditional pattern of referral to a rheumatology department is significantly altered by reducing the non-inflammatory load, then the new to follow-up ratio will inevitable worsen. This is because, as we and others have shown (2,3) patients with non-inflammatory conditions tend to be “one-stop” and those with RA in particular are now tied into continuing follow-up by recent NICE guidelines. There may be other factors influencing the fall-off in referrals from Bexley PCT. In addition to the community clinic provision the PCT has instituted a referral policing system run by the GPs themselves which has applied significant pressure to reduce the numbers of referrals made. This approach has not been adopted by the other local PCTs. However this is not going to affect obligate referrals. The breakdown is shown below. Just as internal referrals are unmonitored (as well as being expected and convenient), referrals of patients between private sector and NHS are likewise independent of any GP input. There is significant patient pressure applied by those who require re-referral and wish to see the same consultant (although we have some evidence that the Choose and Book system is interfering with this common-sense approach, this forms the largest group). Transfers from other hospitals are inevitably arranged for geographical convenience. Hospital staff and staff family members will often make a specific request to see a specific consultant. The 3 cases listed as self requests were one local GP and two people (out of area) who requested an appointment having heard ANB on Radio 4 in a programme with Mark Porter. ANB was the only consultant in the local area who was authorised to see children. Discussion Our results demonstrate that the provision of a specific additional service in a locality will significantly affect referrals to existing services. The proportion of patients coming from the immediate locality dropped by one-fifth (two-fifths of unqualified referrals). Although this resulted in empty clinics initially, new slots were filled by increased numbers of referrals from out of area. The local PCT will have observed a reduction in costs (the community service is off tariff). However, the overall local health economy will not show any reduction as throughput remains unchanged. In other words, the effect of establishing a new service is simply to increase capacity and any spend on the new service will be additional to existing spend. Patients may be disadvantaged by such approaches. The increased numbers of patients coming from outside the “home” PCT implies that they will have longer travelling times to clinics. As, however, the casemix pattern of these referrals appears to be traditional, it is not likely to have a significant long-term effect on patient journeys as a standard proportion will remain “one-stop” patients. A PCT developing a standalone service for non-inflammatory conditions will however have inevitably to accept that the new:follow-up ratio in the local hospital department will deteriorate, as the proportion of inflammatory joint disease patients seen there, and requiring long-term follow-up, will increase. Many hospital departments have been put under pressure to reduce follow-ups on the basis that their ratio compares unfavourably with another hospital. Such comparisons are meaningless if a casemix comparison is not included (2) and are anyway unacceptable if NICE guidelines require a minimum of annual follow-up appointments. Since collecting these data Bexley PCT has established a formal musculoskeletal referral management system (CATS) which requires submission of a standardised form for triage. It is not clear at present how many referrals are being made direct to hospital departments (rheumatology, physiotherapy & orthopaedics) or to the community rheumatology service but initial analysis suggests (again as has been found elsewhere) that the majority of referrals to the CATS are for orthopaedic problems and for back pain. It seems unlikely therefore that it will have any significant impact on the rheumatology service. However there does appear to be a rebound increase of onward referral to rheumatology of “difficult” problems. This may offset the withdrawal of work to the community service – and others have suggested that the development of a CATS actually increases, rather than reduces, overall referral numbers, We will be auditing this at a later date. Map showing local PCT areas. The two outpatient departments within Bexley PCT are shown in red (QMS) & black (EH) Data collection All new patients referred to one of the two Queen Mary’s Hospital consultants (ANB) in the year starting February 2008 (the start point of the community service) were entered during each new patient clinic into the department spreadsheet and categorised by Primary Care Trust (PCT) of origin (total 506; 501 listed by PCT). A note was made of any special circumstances (for example, if a patient was a staff member or relation, where patients were referred internally by other hospital consultants or staff, referrals from other hospitals, re-referrals and referrals for a second opinion, transfers from the private sector). These were termed obligate referrals. Method From the spreadsheet, numbers and percentages of new patients from each PCT were calculated. These were recorded both unsorted and subdivided into unqualified (ie completely new GP originated referrals) or obligate. The figures were then compared with our retrospective data on 1150 long-term follow-up patients (average follow-up time 9.55yr for RA, 5.94yr for other inflammatory conditions), which represents a stable indicator of PCT of origin. • Conclusion • Development of a PCT based CRC alters local referral patterns but does not result in a reduction of hospital work • Spare clinic capacity resulting from reduced local referral will be taken up by more distant referrals, largely through Choose & Book • Withdrawal of non-inflammatory problems from a hospital department will adversely affect new:follow-up ratios References 1. Bamji AN, Dieppe P, Haslock I, Shipley ME What do Rheumatologists do? A Pilot Audit Study. Br J Rheumatol 1990, 24, 295-8 2. Litwic A, Bamji AN. Follow-up or discharge? A new patient outcome analysis. BSR Annual Meeting, 2008 (Abstract 417 ii121) 3. Holroyd CR, Fletcher MJ, Ledingham J. Variation in case mix across Wessex rheumatology units over 10 years. BSR Annual Meeting 2009 (Abstract 263, i109) Correspondence: andrew.bamji@nhs.net




![[PDF] Free Download Kill the Queen By Jennifer Estep](https://cdn4.slideserve.com/8030381/slide1-dt.jpg)
![[Download] Kill the Queen By Jennifer Estep PDF eBook](https://cdn4.slideserve.com/8295146/slide1-dt.jpg)
![[PDF] Free Download Kill the Queen By Jennifer Estep](https://cdn4.slideserve.com/8476870/slide1-dt.jpg)