Download
1 / 50
520 likes | 997 Views
The Management of the First Seizure. Dr.Laura Martin . Aims. To have an understanding of the common causes of a first seizure presenting to the Emergency Department To have an understanding of the basic management of the first seizure To have some basic rules for seizure management.

E N D
The Management of the First Seizure Dr.Laura Martin Dr Laura Martin (with a little bit of help from Tony Holley)
Aims • To have an understanding of the common causes of a first seizure presenting to the Emergency Department • To have an understanding of the basic management of the first seizure • To have some basic rules for seizure management Dr Laura Martin (with a little bit of help from Tony Holley)
Definition of Seizure An episode of abnormal neurological functioning caused by abnormal discharge of neurons! Dr Laura Martin (with a little bit of help from Tony Holley)
Classification of Seizures • Generalised - loss of consciousness • Partial - no loss of consciousness • Unclassified Dr Laura Martin (with a little bit of help from Tony Holley)
Generalised Absence Tonic Clonic Myoclonic Clonic Tonic Atonic Partial Simple Partial Motor Sensory Autonomic Complex Partial With psychic, cognitive or affective symptoms With automatism's Partial seizures with secondary generalisation Classification of Seizures Dr Laura Martin (with a little bit of help from Tony Holley)
Classification of Seizures by Etiology • Acute Symptomatic seizures • Remote Symptomatic seizures • Idiopathic Dr Laura Martin (with a little bit of help from Tony Holley)
CNS infections Meningitis Encephalitis Abscess Vascular disease CVA Vasculitis Trauma Hypertensive Eclampsia Neoplasms Benign Malignant - Primary, Secondary Metabolic Electrolyte disturbances Hypoglycaemia Hypoxia Renal Failure Acute Symptomatic seizures Dr Laura Martin (with a little bit of help from Tony Holley)
Tricyclic antidepressants Antidepressants Theophylline Withdrawal - ETOH, benzo’s Anticholinergics Organophosphates Cocaine Amphetamines Lignocaine Anti -psychotics Antihistamines Isoniazid Acute Symptomatic seizures- Toxin Drugs Dr Laura Martin (with a little bit of help from Tony Holley)
Remote Symptomatic Seizures • Previous head injury • Previous CVA • Congenital CNS disorders • Previous hypoxic injury • Previous CNS infections • Degenerative diseases Dr Laura Martin (with a little bit of help from Tony Holley)
Incidence & Epidemiology • 5% of the population have a seizure some time in their life • Bimodal frequency • adult 1st generalised seizure accounts for 1% ED visits Dr Laura Martin (with a little bit of help from Tony Holley)
Causes of seizures presenting to Emergency Departments Cause Sempere et al 1992 Henneman et al 1994 Idiopathic 27.6%44.0% Infarction 23.5%11.0% Cerebral Cystercercosis - 12.0% ETOH 11.2% - CNS infections 9.2%10% CNS tumour 8.2%7.0% Vascular Malformation 6.1% - Trauma 4.1% 4.0% Drug toxicity 3.1% - Hyponaetraemia 2.0% 2.0% Systemic Infection - 2.0% Other 5.0% 9.0% Dr Laura Martin (with a little bit of help from Tony Holley)
Causes of seizures by age Cause Age < 45 years Age > 45 years Idiopathic 45%15.5% Infarction 2.5% 37.9% ETOH 15% 8.6% CNS infections 17.5% 3.4% CNS tumours 2.5% 12% Vascular Malformation 7.5% 5.2% Trauma 7.5% 1.7% Drug toxicity 0% 5.2% Other 2.5% 10.2% Sempere et al 1992 Dr Laura Martin (with a little bit of help from Tony Holley)
Causes of seizures by age - acute symptomatic seizures • 6/12 to 5 years -Febrile convulsions • Young adults -Trauma 26% -Drug withdrawal 20% • Elderly - CVA 44% Annegers et al 1995 Dr Laura Martin (with a little bit of help from Tony Holley)
Differentiated Febrile convulsion Idiopathic epilepsy Acute symptomatic seizures Remote Symptomatic seizures Undifferentiated Cardiac Arrhythmia's Vasovagal Episode Cardiac - Structural Blood loss Postural Hypotension Sepsis Psychogenic etc Presentation to the Emergency Department Dr Laura Martin (with a little bit of help from Tony Holley)
Presentation to the Emergency Department • Has the patient had a seizure? • What kind of seizure was it? • Was there a focal component? • Was this the first seizure? • Is there a family history of seizure disorder? • Why did the seizure occur? Dr Laura Martin (with a little bit of help from Tony Holley)
Other Important History • Systemic illness • drug use/abuse • pregnancy • mental retardation • head injury • unexplained bruises/tongue biting • nocturnal enuresis • precipitants Dr Laura Martin (with a little bit of help from Tony Holley)
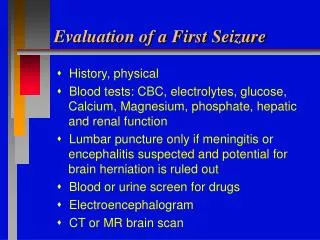
Management • Historical documentation of the seizure • Physical examination • Investigations • Cessation of seizures • Observation • Disposal • Advice • Seizure Prophylaxis • Follow up Dr Laura Martin (with a little bit of help from Tony Holley)
Investigations Dr Laura Martin (with a little bit of help from Tony Holley)
Rule Always do a glucose on any one who is having a seizure or has had a seizure! Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario 1 • 17 year old girl • Post first witnessed tonic clonic seizure • Been out to a party the night before • Uncle has epilepsy • Now well, GCS 15, Vital signs normal • Neurological exam normal Dr Laura Martin (with a little bit of help from Tony Holley)
Investigations • Glucose • Sodium • Calcium • Consider urine and pregnancy test • CT [ MRI ] & EEG as outpatient Dr Laura Martin (with a little bit of help from Tony Holley)
Post first seizure advice • Management of a seizure at home • Safe activities • Driving • Who should know? • Have I got epilepsy? • Not life threatening • Exacerbating factors • Follow up Dr Laura Martin (with a little bit of help from Tony Holley)
Seizure recurrence • Most common within the first 6 months • More than 50% of those who have recurrence will occur within 6 months • Rate varies from 36 -77% Dr Laura Martin (with a little bit of help from Tony Holley)
Seizure recurrence increased if • Symptomatic Seizure • History of epilepsy in a sibling • Todd’s paralysis • EEG abnormalities • 2 seizures - 80-90% Dr Laura Martin (with a little bit of help from Tony Holley)
RULE Seizure prophylaxis for all first symptomatic seizures Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario 2 • 50 yr old woman • Post tonic clonic seizure • Husband said twitching started in her R arm, then progress to LOC. • History of recent headaches. • Now well, GCS 15, appears neurologically intact • Vital signs normal Dr Laura Martin (with a little bit of help from Tony Holley)
RULE ALWAYS LOOK IN THE FUNDI Dr Laura Martin (with a little bit of help from Tony Holley)
RULE First Focal Seizure = CT scan!!!!!! Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario 3 • 50 yr old woman • Post generalised seizure • Previously well, no seizures in the past • Recent headache for 24 hours, unwell & fever • Now GCS 13, Temp 39.8 • Confused, unco-operative 30 minutes post seizure • Moving all limbs. Dr Laura Martin (with a little bit of help from Tony Holley)
Who to CT? • Focal seizures • trauma • anticoagulants • alcoholics • immunosuppressed • fever,stiff neck,persistent headache • focal neurology Dr Laura Martin (with a little bit of help from Tony Holley)
RULE Do not LP a patient who has a decreased Glascow coma score!! Treat first, CT & ask questions later!! Dr Laura Martin (with a little bit of help from Tony Holley)
RULE A GCS < 13 is a relative contraindication to LP even after a normal CT!! Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario 4 • A 75 yr old man • Previous hypertension • Post tonic clonic seizure • Now GCS 15 but right arm weakness Dr Laura Martin (with a little bit of help from Tony Holley)
RULE Focal neurology = CT scan Focal neurology does not = LP Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario 5 • 18 yr old man • Rugby injury with LOC, scalp laceration • Initially in ED GCS 15, vomited twice and complaining of a headache • Has tonic clonic seizure in ED. Self resolved • Now GCS 12 - 2 minutes post seizure Dr Laura Martin (with a little bit of help from Tony Holley)
RULE Trauma & Seizure = CT scan!! Dr Laura Martin (with a little bit of help from Tony Holley)
Status Epilepticus • Continuous or repetitive seizures without time for recovery • neuronal injury can occur in less than 30min • may be subtle Dr Laura Martin (with a little bit of help from Tony Holley)
RULE • BEWARE THE INTER-ICTAL PATIENT Dr Laura Martin (with a little bit of help from Tony Holley)
Treatment of Status Epilepticus • All patients who still fitting on arrival to ED • fitting for more than 10min • LONGER THE DELAY HARDER TO CONTROL Dr Laura Martin (with a little bit of help from Tony Holley)
0-5 minutes • Confirm diagnosis • Oxygen • Airway & Breathing [ Consider ETT ] • Vital signs • IV access • Glucose check • Oximetry • Lab Dr Laura Martin (with a little bit of help from Tony Holley)
5-10 minutes • If hypoglycaemic treat • Adults 100 mg thiamine followed by 50 mls 50% glucose • Children 2 mls/kg 25% Dr Laura Martin (with a little bit of help from Tony Holley)
10-20 minutes • 0.1 mg/kg lorazepam at 2mg/min up to 4 mg total or • 0.2 mg/kg diazepam at 5mg/min up to 20mg/min Diazepam must be followed by a loading dose of phenytoin Dr Laura Martin (with a little bit of help from Tony Holley)
Difficult access? • IM midazolam 10mg • PR diazepam 0.5 mg/kg • PR lorazepam 0.1mg/kg Dr Laura Martin (with a little bit of help from Tony Holley)
20+ minutes • Load with phenytoin 20 mg/kg no faster than 50 mg/min in adults and 1mg/kg/min in children • IV fluids must be N Saline Dr Laura Martin (with a little bit of help from Tony Holley)
If Status continues • 1. Additional phenytoin 5 mg/kg up to a total of 30 mg/kg • 2. Midazolam load 0.2 mg/kg infusion • 3. Phenobarbitone 20mg/kg at max 100mg/min • 4. Proprofol load with 0.2mg/kg then infusion • Expect apnea • Intubation will be required - rapid sequence induction with thiopentone and suxamethonium Dr Laura Martin (with a little bit of help from Tony Holley)
Scenario • 25 year old woman • OD 30 amitryptiline tablets • brief generalised seizure en route • now GCS 14 P120 BP 110/60 Dr Laura Martin (with a little bit of help from Tony Holley)
RULE • Phenytoin no use for toxicological induced seizures Dr Laura Martin (with a little bit of help from Tony Holley)
Acute Symptomatic Seizure requiring ongoing treatment & investigation Febrile seizure where underlying cause needs treatment or fever does not settle Focal seizure Status epilepticus or prolonged seizure. Recurrent seizures Social Situation Admission criteria for a first seizure Dr Laura Martin (with a little bit of help from Tony Holley)
Conclusion No one seizure is the same The clinician must always think of the underlying cause & investigate & treat appropriately Dr Laura Martin (with a little bit of help from Tony Holley)
References • Em Clinics N America Feb 1999 17;1 • Emergency medicine reports Vol 18;14 1999 • Neurology Nov 1999 S4 • Lancet July 2000 Vol 356 Dr Laura Martin (with a little bit of help from Tony Holley)