Download
1 / 44
5.58k likes | 17.58k Views
Celiac Disease. (gluten-sensitive enteropathy ). Introduction. Celiac Disease is a chronic disease of the digestive tract. It interferes with the digestion and absorption of food nutrients. People with celiac sprue cannot tolerate gliadin , the alcohol-soluble fraction of gluten

E N D
Celiac Disease (gluten-sensitive enteropathy)
Introduction • Celiac Disease is a chronic disease of the digestive tract. • It interferes with the digestion and absorption of food nutrients. • People with celiac sprue cannot tolerate gliadin, the alcohol-soluble fraction of gluten • Celiac disease is caused by an autoimmune reaction to gluten. • The root cause of celiac disease is unknown, but inheritance is a risk factor. • Celiac Sprue is a lifelong disease, and if untreated it is associated with increased mortality .
What Is Gluten ? • “Gluten” is a general term for a composite of the storage proteins gliadin and glutenin. • These proteins (conjoined with starch) comprise 80% of the total protein in wheat/rye/barley seed . • Corn (maize), sorghum, and rice are considered safe for a patient to consume. They do contain types of gluten that do not trigger the disease
Frequency • Approximately 3 million people in Europe and another 3 million people in the United States are estimated to be affected by celiac sprue. • The highest prevalence of celiac sprue is in Ireland and Finland and in places to which Europeans emigrated, notably North America and Australia. • The incidence of celiac sprue is increasing among certain populations in Africa, Asia (India),and the Middle East.
Celiac disease can be seen first time in any part of life. • Usually, this disorder can be discovered in childhood .
Pathophysiology • Celiac Disease has a strong hereditary component. • The prevalence of the condition in first-degree relatives is approximately 10%. • A strong association exists between celiac sprue and two human leukocyte antigen (HLA) haplotypes (DQ2 and DQ8). • Damage to the intestinal mucosa is seen with the presentation of gluten-derived peptide gliadin, consisting of 33 amino acids. • Helper T cells mediate the inflammatory response.
People with celiac disease have abnormally high levels of associated antibodies like: anti-gliadin, which unite with antigens (toxic amino acid sequences) that are found in wheat, rye, and barley. • In people with celiac disease, the immune system treats gluten as a foreign invader and produces elevated levels of antibodies to get rid of it, causing symptoms and associated discomfort. • As a result, intestinal villi gets damaged (shortening and villous flattening)
How does gluten cause negative effects? • Certain Pro- and Gln-rich gliadin peptide fragments survive the digestion process & make it to the gut • These peptides are deamidated by tissue transglutaminase (tTGase) • APCs in HLA-DQ2 or –DQ8 positive individuals express these deamidated peptide fragments on class II MHC molecules • The resulting CD4+ T-cell mediated immune response can eventually result in the development of celiac disease
Therefore, the only currently recognized treatment for celiac disease is complete abstinence from food grains containing gluten proteins .
Risk Factors • Having a risk factor for Celiac Disease makes the chances of getting a condition higher but does not always lead to Celiac Disease • Celiac Disease can be associated with disorders such as thyroid disease, Anemia of unknown cause, type I diabetes or other autoimmune disorders. • Family history of Celiac or autoimmune disorders.
Race:Celiac sprue is most prevalent in Western Europe and the United States. The incidence is increasing in Africa and Asia. • Sex: Incidence of celiac sprue is slightly higher in females than in males. • Age:The age distribution of patients with celiac disease is bimodal, the first at 8-12 months and the second in the third to fourth decades. The mean age at diagnosis is 8.4 years (range, 1-17 y).
Italian race: celiac is common in Italy and descendents. • Large amounts of gluten at weaning are associated with an increased risk for developing celiac disease. • Finally, repeated rotavirus infections in infancy appear to be associated with a higher risk of developing celiac disease autoimmunity in genetically predisposed individuals
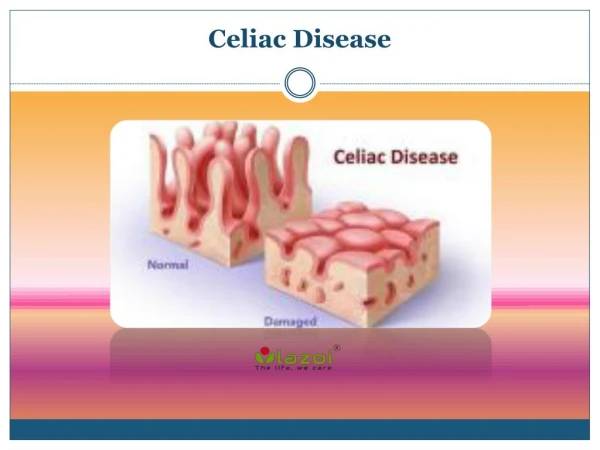
Histology of Celiac Disease • The histological lesion of gluten sensitivity primarily affects the proximal small bowel. • the damage caused by celiac disease can be more extensive than once thought, and that it likely affects the entire small bowel, rather than just the lamina propriaand crypt regions. • The lesion is described as subtotal villus atrophy.
The difference between normal (left) and abnormal (right) Mucosa
We can see counts of lymphocytes and plasma cells in lamina of damaged Mucosa
Symptoms • Celiac Disease has wide spread symptoms. • The list of signs and symptoms ofCeliac Disease includes about 35 symptoms . • Symptoms in children may differ from them in adults.
The most common symptoms in adults are : 1-abdomenal pain 2-Diarrhea 3-Pale stools 4-Weight loss 5-Dehydration
The most common symptoms in children are : 1-Delayed growth 2-irritability 3-Anemia 4-Weight loss 5-Bloating abdomen
Older children with celiac disease who present with GI manifestations may have onset of symptoms at any age. • The variability in the age of symptom onset possibly depends on the amount of gluten in the diet and other environmental factors
Signs • Physical findings depend on extent of celiac disease. • Celiac disease may occur in asymptomatic individuals without any positive clinical findings • Bloating of the abdomen is a relatively common finding . • Dry mucosal membranes with vomiting or diarrhea indicate the degree of dehydration.
Some extraintestinal manifestations of celiac disease can be shown in some patints. • The most common signs we can see are: 1-weight loss 6-peripheral neuropathy 2-fluid retention 7-infertility 3-anemia 8-muscle weakness 4-osteoporosis 5-bruising easily
Complications • Dermatitis herpetiformis: • A blistering skin rash that involves the elbows, knees, and buttocks are associated with dermal granular IgA deposits . • Dermatitis herpetiformis is a rare occurrence in childhood and is described almost exclusively in teenagers and adults.
Dental enamel hypoplasia: • These enamel defects involve only the permanent dentition and may be the only presenting manifestation of celiac disease. • Often, GI symptoms are minimal or absent.
Short stature and delayed puberty: • 10% of children with idiopathic short stature may have celiac disease that can be detected on serologic testing. • Adolescent girls with untreated celiac disease may have delayed onset of menarche.
Arthritis and arthralgia: • Arthritis can be a common extraintestinal manifestation of adults with celiac disease, including those on a gluten-free diet. • 3% of children with juvenile chronic arthritis may have celiac disease.
Psychiatric disorders: • celiac disease can be associated with some psychiatric disorders, such as depression and anxiety. • These conditions can be severe and usually respond to a gluten-free diet.
Diagnosis • First, a thorough physical examination is conducted, including a series of blood tests. • Second, a duodenal biopsy is performed with multiple samples from multiple locations in the small intestine. • And third,thegluten-free diet is implemented
Physical Examination: 1-pallor (due to anemia) 2-hypotension (low blood pressure) 3-edema (due to low levels of protein, [albumin] in the blood) 4-dermatitis herpetiformis (skin lesions)
5-easy bruising (lack of vitamin K) 6-loss of various sensations in extremities including vibration, position and light touch (vitamin deficiency) 7-signs of severe vitamin/mineral deficiencies which may include: -diminished deep tendon reflexes -muscle spasms
Serologic Tests • EMA(Immunoglobulin A anti-endomysium antibodies) • AGA (IgA anti-gliadin antibodies) Some people do not produce IgA antibodies. • DGP (Deamidatedgliadin peptide antibody) • tTGA (IgA anti-tissue transglutaminase)
Biopsy • It is the key of diagnosis. • a biopsy of the small intestine [jejunal] is called for. • the tissue samples are examined under a microscope for signs of injury
The biopsy can be taken by inserting a tube through the mouth and throat
Normal Celiac Disease
Under the microscope, we see the atrophy of Mucosa and Elevated numbers of T-cell lymphocytes . • The small bowel biopsy samples of persons with dermatitis herpetiformis often show similar damage.
Prognosis • The prognosis for patients with correctly diagnosed and treated celiac sprue is excellent. • The prognosis for patients with celiac sprue who are not responding to gluten withdrawal and corticosteroid treatment is generally poor. • Mortality is usually associated with water and electrolyte depletion.
Treatment • There are two main ways to treat and control celiac disease: 1- Diet 2- Corticosteroids
Diet: • Complete elimination of gluten-containing grain products, which include wheat, rye, and barley, is essential to treatment. • After an initial period of avoidance, oats might be reintroduced into the diet of patients with celiac disease. • These patients should be monitored carefully for recurrent symptoms.
Gluten-free food These days you can find meals made especially for celiac disease patints, which have no gluten content.
Corticosteroids: • Corticosteroids have anti-inflammatory properties and cause profound and varied metabolic effects. • These agents modify the body's immune response to diverse stimuli.
Prednisone: Can be used in patients with refractory celiac sprue • Adult: 30-40 mg/d PO; taper off completely in 6-8 wk • Pediatric: 1 mg/kg/d PO; not to exceed 30 mg/d; taper off completely in 6-8 wk
The End By: UsefBada