Download
1 / 26
480 likes | 1.24k Views
Lung Pathology TUBERCULOSIS. TUBERCULOSIS. Definition: Chronic infective granuloma caused by tubercle bacilli Causative organism: Two types of bacilli infect man: Human and Bovine Its growth is strict aerobic and inhibited by acidic ph

E N D
TUBERCULOSIS Definition: Chronic infective granuloma caused by tubercle bacilli Causative organism: Two types of bacilli infect man: Human and Bovine Its growth is strict aerobic and inhibited by acidic ph It has no known exotoxins, endotoxins or histolytic enzymes It consists of complex lipid, carbohydrate around tuberculoprotein The bacteria is non-motile and are carried by macrophages to spread by various methods
TUBERCULOSIS Methods of infection: Inhalation: is the commonest method The human bacilli are inhaled in coughed droplets or dust contaminated with sputum from a case with opened TB The inhaled bacilli infect the tonsils or the lung Most infections are acquired by sustained exposure rather than casual contact Ingestion: of raw milk contaminated with bovine or human bacilli. They infect the tonsils or intestine Skin inoculation: by handling infected material. This method is not common
Microscopic Picture of Tubercles 1-Epithelioid cells: With abundant pale red cytoplasm, indistinct cell borders and round or oval vesicular nuclei 2- Langhan’s giant cells 3- Lymphocytes 4- Central caseation
Tuberculosis Clinical patterns Primary type: occurring in individuals following the initial infection, this type is called childhood type, as it is frequent in children leading to formation of primary complex Post primary (secondary type): tend to be more chronic and slowly progressive. It is associated with significant (although inadequate) resistance
Primary Tuberculosis Primary complex Sites: Tonsil Lung Intestine Skin
Primary Pulmonary Complex Ghon’s Focus Under the pleura, small in size (1cm) with late caseation Tuberculous lymphangitis Tuberculous lymphadenitis
Fate of Primary Complex I-Healing Fibrosis & calcification Very small foci Bacilli may persist for life II- Spread: low immunity 1- Direct:focus enlarges and gives new lesions with extensive caseation 2- Haematogenous Small No of bacilli Moderate number of bacilli Large number of bacilli Miliary TB 3- Bronchial spread III- Encapsulation and reactivation
Secondary Tuberculosis This type of tuberculosis arises in a previously sensitized individual, whether the TB bacilli are derived from endogenous or exogenous sources Most cases of secondary TB represent reactivation of asymptomatic primary disease The reactivation is the result of shift in the balance between host and organism due to such factors as reduced immunity, poor nutritional status, alcoholism or advanced age
Secondary Pulmonary Tuberculosis Apical lesion Are almost always near the apex of the lung at sites of high oxygen tension (where the bacilli had localized at the time of original bacillemia) The minimal lesion at the apex consists of 1-3 cm focal area of caseous consolidation, usually within 1 -2cm from pleural surface TB cavities with caseation
Secondary Pulmonary Tuberculosis Course of Apical lesion a) Healing, scarring and calcification giving fibrocalcific 'arrested‘ tuberculosis b) Progressive local spread: Fibrocaseous foci may undergo softening and erode through airways and emptying of this soft material into the bronchus (open case) eaving a cavity lined by caseous material and surrounded by fibrous tissue (Chronic fibrocaseous T.B) Retrograde spread of caseous material through the distal airways produce small caseating (acinar lesions) mainly at the base of the ung. These lesions subsequently fuse into larger lesion
The lung shows a rounded apical cavity (4x3cm.) having fibrous wall and yellow caseous lining. multiple yellow caseous foci Diagnosis: Chronic fibrocaseous pulmonary tuberculosis. Chronic firocaseous TB
The lung shows a rounded apical cavity (8x7 cm.) having fibrous wall and yellow caseous lining. The lower lobe shows 2 small cavities and multiple yellow caseous foci The pleura shows fibrosis and adhesions Diagnosis: Chronic fibrocaseous pulmonary tuberculosis. Pleural adhesions
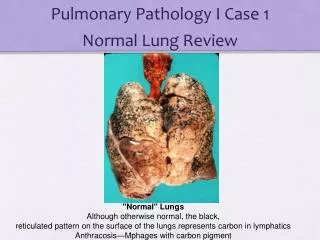
The lung shows multiple scattered small yellow caseous foci. Diagnosis: Miliary tuberculosis of the lung.
lung shows multiple scattered small yellow caseous foci. The lymph nodes are enlarged with yellow caseous foci. The pleura shows fibrosis and adhesions. Diagnosis: Miliary tuberculosis of the lung. Pleural adhesions.
Parts of lumbar vertebrae. Two vertebral bodies and their disc are destroyed by yellow caseous material which collects under the anterior ligament (cold abscess). There is a fracture between the two vertebrae. Diagnosis: Pott’s disease. (tuberculosis of vertebrae)
Section in a lymph node shows multiple tubercles formed of : 1-Epithelioid cells having pale cytoplasm, round or oval vesicular nuclei and indistinct cell border 2- Langhan’s giant cells with large number of round nuclei arranged in the periphery as a circle or arch 3- Lymphocytes encircle the tubercle. 4- The center of the tunercle may show pinkish granular structureless areas of caseation. Diagnosis: Tuberculosis of lymph node
Section in lung tissue having mutiple small tubercles formed of epitheliid cells, Langhan’s giant cells and lymphocyte with minimal central caseation. The alvolar wall are congested. Diagnosis: Miliary tuberculosis, lung
Section in the lung shows large irregular areas of caseation appearing granular or homogenous pink, surrounded by tuberculous reaction and fibrous tissue. Some alveoli show haemorrhagic exudate and others show compensatory emphysema. Diagnosis: Chronic fibrocaseous tuberculosis, lung. Caseation Fibrosis