Download
1 / 83
1.09k likes | 2.14k Views
Body Fluid Compartments. Free interactive Physio tools http://www.winona.edu/biology/adam_ip/home/. Lecture outline. I. Water compartments of the body A.Intracellular B. Extracellular i. Interstitial ii. Plasma iii. Transcellular II. Compare/contrast water compartments

E N D
Body Fluid Compartments Free interactive Physio tools http://www.winona.edu/biology/adam_ip/home/
Lecture outline I. Water compartments of the body A.Intracellular B. Extracellular i. Interstitial ii. Plasma iii. Transcellular II. Compare/contrast water compartments A. Size B. composition C. Osmolality III. How do we have different composition/ movement of solutes A. Different permeability B. Types of transport across the membrane for solutes--Protein transporters C. Review of Simple diffusion of solutes IV. Movement of water A. Osmosis-movement across cell membranes due to unequal particles B. Hydrostatic pressure- movement across capillaries V. Examples of when water vs. solute moves VI. Definition of osmotic pressure A. Examples of osmotic pressure differences in body fluid compartments VII. Tonicity vs osmolality A. Examples of tonicity and osmolality
Body Fluid Compartments • Why do you need to understand body fluid compartments and osmolarity calculations? • Many of you will be applying IV care for patients, and sometimes doctors make mistakes, so you need to be able to catch these errors. • Most medical solutions are calculated in units that don’t require a periodic table of elements, but if someone miscalculates a solution, and you inject it, and the patient crashes, you are just as liable, and you will be sued.
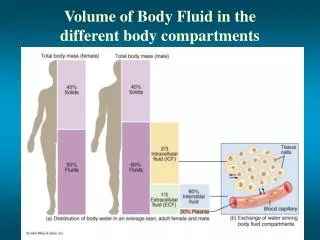
Water • Water makes up 60% of our body weight • Divide this into two compartments • Intracellular water • Extracellular water
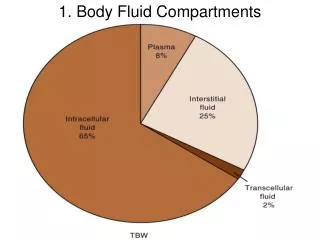
Compartments * Lumen of stomach These are stomach epithelial cells • Intracellular Fluid (60% Body Wt) • Extracellular Fluid • Interstitial fluid(the water immediately outside cells, between and around cells) (30%) • Plasma fluid(the water inside blood vessels, but not in blood cells) (9%) • Transcellular fluid(the water enclosed in chambers lined by epithelial membranes) (1%) * * *
Body Fluid Compartments • If you manipulate one body fluid compartment, it has an effect on another compartment. • Body fluid compartments have different sizes and volumes, and different compositions. • Although the volume and substances dissolved in the fluid of one compartment is different than another compartment, each compartment has the same number of particles dissolved in the water.
Body Fluid Compartments • Therefore, size and composition (what particles are dissolved in the water) does not have an effect on the number of particles dissolved in the water of each compartment. • If you could count every particle dissolved in the water of that compartment, you would see that in all the compartments there are the same number of particles: 300 million particles per liter, expressed as “300 million osmoles” or “300 mili-osmoles”. • It could also be described as having “an osmolarity of 300”.
Body Fluid Compartments • That means that there are 300 million particles (or 300 milliosmoles, abbreviated 300 mOsm) dissolved in each liter of water in each compartment. • If one compartment has more particles than another one next to it, and if those particles cannot reach equal numbers on their own because the cell membrane blocks their passage, water will try to dilute the compartment with the higher number of particles until they are at the same number of particles per liter. • Water always moves across the compartments because cell membranes always allow water to pass.
Body Fluids compartments • Different compositions (different amounts of individual particles). For example, one coffee cup has 1 teaspoon of instant coffee and 2 teaspoons of sugar, another cup has 2 teaspoons of coffee and 1 teaspoon of sugar. • Different volumes(one coffee cup holds 8 oz, another holds 16 oz) • Same osmolalities (total number of particles) When you evaporate away the liquid in both coffee cups and count each coffee grain and each sugar grain, there are 300 million total grains per liter in both cups. 0.3 Osmolal = 300 mOsmolal (actually closer to 280mOsmolal) Plasma Interstitial Intracellular
Diffusion • If the plasma becomes diluted to 260 mOsm, and the cells next to a blood vessel are still at 300 mOsm, the cells now have more particles. By a law of physics, all particles want to move from an area of high concentration to an area of low concentration…That is why perfume will diffuse out of the bottle and fill up the room if you leave the top off. • Therefore, since the particles in the cells are 300 mOsm and the particles in the blood vessel are 260 mOsm, which way do the particles want to move? • The particles in the cells will want to move into the plasma. • However, the cell membranes will not allow them to pass, so they are stuck inside the cell. • The next force of nature that will kick in is water diffusion. Water also wants to move from its area of high concentration to an area of low concentration.
Diffusion • If I have 2 identical cups with the same amount of water, and I add 20 teaspoons of lemonade to one cup and 10 teaspoons of lemonade to the other cup, which cup is more concentrated with lemonade? The one with the most particles (20 teaspoons). Which one is more concentrated with water? The one with the fewest particles (10 teaspoons). • If these two solutions were in body fluid compartments that were next to each other, and if the particles cannot move from their area of high concentration to low concentration, then water will move from its area of high concentration (which was the more watery cup; the one that had only 10 teaspoons of lemonade) to its area of low concentration (the cup with low WATER concentration was the one with 20 teaspoons of lemonade). • That is the same thing as saying that particles suck water.
Diffusion • What will move, in order to dilute the cells? Water. Why? Because particles suck! • In the case where the plasma has 260 mOsm (260 particles per liter) and the nearby cells have 300 mOsm (300 particles per liter), will the cells will draw the water into themselves, or will the plasma draw water into the blood vessel? • The compartment with more particles (the cells) will suck the water in. Therefore, water will move from the plasma to the adjacent cells. • What will that do to the cells? They will lyse (rupture). • When would that ever happen in real life?
Diffusion • When would that ever happen in real life? • January 12th, 2007, A 28 year-old mother of three from Sacramento decides to go on a radio program to compete in a contest called, “Hold your Wee for a Wii.” They offered a prize to the person who could drink the most water in two hours without going to the bathroom. • During this contest, she drank 6 liters in 2 hours (3 liters an hour). The maximum the kidney can filter is 1 liter an hour. • After the contest, she called her co-workers to say she wasn’t coming to work because her head hurt so badly. • Later she is found dead.
Diffusion • She was OVER hydrated, so the original 300 particles per liter in her plasma were now at 300 particles per 2 liters, since the excess water increased her blood volume. • That means there were only 150 particles per liter, so overall, there were now fewer particles in the plasma than in the adjacent cells. • Therefore, the adjacent cells had more particles, and they sucked in the water. • Her brain cells also sucked up the water until they ruptured and exploded in her skull.
Overhydration • Drinking too much water changes the extracellular osmolality. • When the plasma is too dilute (too much water, too few solutes), water will leave the bloodstream to enter the tissues, where there are more solutes (solutes SUCK!). • Water will enter the tissues (intracellular body fluid compartment), including the brain. • The excess water will cause the brain to swell.
Overhydration • Thus, we learn that if a person is over-hydrated, the plasma will be diluted below 300 mOsm, but the cells still have 300 mOsm in particles. • So, the cells will draw in more water from the plasma and the cells will enlarge and rupture. • She should have been given an IV that was hypertonic (greater than 300 mOsm) to balance out the number of particles in the plasma so it matched the number of particles in the cells.
Dehydration • The opposite is true for someone who is dehydrated. • Since the original number of particles was 300 million particles per liter, and then the patient became dehydrated, they would now have 300 million particles per half a liter (since they lost plasma volume due to dehydration), so their plasma is actually at 600 mOsm per liter. • Therefore, if a patient is mildly dehydrated, you will give an IV that was hypotonic (less than 300 mOsm, be careful of the drip rate) to balance out the number of particles per liter within the plasma and within the adjacent cells. • This has the same effect as having the patient drink some water, but the iv will work faster.
Dehydration • If a doctor accidentally tells you to give a mildly dehydrated patient an IV solution that is hypertonic (greater than 300mOsm), the plasma will have more particles than the cells, and the cells will have the water sucked out of them, which also causes death. • Hypertonic solutions are only okay for an overhydrated person, or a dehydrated person who has lost particles, such as from blood or electrolyte loss after surgery. • Understanding body fluid compartments is important!
Sources of water intake/output Water intake must equal water output 2500 ml 2500 ml
Thirst mechanism for regulating water intake Na+ acts as a powerful water magnet, but the kidney and brain hormones can regulate water independently of Na+. Drinking water satisfies thirst before the water is absorbed because the mouth, throat, and stomach sensors provide feedback signals that inhibit the thirst center in the brain.
Types of Dehydration • Isotonic fluid deficit • Hypotonic fluid deficit • Hypertonic fluid deficit
Isotonic fluid deficit • Type of Loss: solute and water loss proportional, no change in plasma volume, serum sodium level is decreased to 125-150 mEq/L. The cause of the fluid loss is GI fluid loss (vomiting or diarhea), urine loss and decreased oral intake.Clinical signs: poor skin turgor; cold, dry dusky skin; sunken eyes; dry mucous membranes; depressed fontanelles in babies; rapid pulse; low B/P; irritability or lethargyFluid Replacement Guidelines: Initially, a bolus of 0.9% sodium chloride or Ringer's lactate is given followed by 5% Dextrose in water and 0.45% sodium chloride. Half of the deficit should be replaced in the first 8 hours and the remaining half over the next 16 hours
Hypotonic fluid deficit • Type of Loss: More solute is lost than water. Plasma volume moves from the ECF to the ICF. Serum sodium levels are decreased below 125 mEq/L. The cause of the fluid loss is often a GI fluid loss with hypotonic oral intake.Clinical Signs: Include very poor skin turgor; cold, clammy, dusky skin; sunken eyes; slightly dry mucous membranes; depressed fontanelles in babies; rapid pulse; very low blood pressure; lethargy; coma; seizuresFluid Replacement Guidelines: Initially a bolus of 0.9% sodium chloride or Ringer's Lactate followed by 5% Dextrose in water and 0.9% sodium chloride. If the patient is severely symptomatic 3% sodium chloride at 4mL/kg should be given over 10 minutes with close monitoring. Half of the fluid deficit should be replaced in the first 8 hours and the remaining half over the next 16 hours.
Hypertonic fluid deficit • Type of Loss: There is greater water loss than solute loss. Volume moves from the ICF to the ECF. Sodium levels are maintained at over 150 mEq/L. The cause is GI fluid loss with hypertonic oral intake, diabetes insipidus, fever and hyperventilation.Clinical Signs: Include fair skin turgor; cold, thick and doughy skin; sunken eyes; parched mouth; depressed fontanelles in babies; a moderately rapid pulse; moderately low blood pressure; hyperirritability; high-pitched crying in babies; seizures.Fluid Replacement Guidelines: 5% Dextrose in water and 0.225% or 0.45% sodium chloride. If the patient is hypertensive 0.9% sodium chloride or Ringer's lactate should be given at a rate of 20mL/kg over one hour. Fluid replacement should be given slow and gradual over 48 hours. 2 to 3 mEq/kg of potassium should be given per 24 hours. At least 2 mEq/L/hour of sodium should also be included in the IV fluids that are used.
Patient Case 1 • Patient recovering from bacterial infection has been suffering with diarrhea. He has not been able to eat or drink anything. Low BP=70/40, High Pulse-110bpm. • Do you give an iv solution that is hyper, hypo, or isotonic? Why?
Patient Case 1 • Give Isotonic solution (ringers solution). • The person has a high pulse rate and low blood pressure. • Since the person is severely dehydrated, but the water loss and particle loss are equal (diarrhea or vomiting) you do not want to overhydrate the cells with a hypotonic solution and you don't want to make the dehydration worse by giving him a hypertonic solution, thus you give him an isotonic solution.
Patient Case 2 • Patient, age 24, has been suffering from food poisoning with vomiting and diarrhea. He has been drinking a lot of plain water, not Gaitoraid or Pedialite. • Skin and mucous membranes are dry, and he's complaining of a headache. Heart rate is normal, but he has high BP=200/120. • Do you give an iv solution that is hyper, hypo, or isotonic? Why?
Patient Case 2 • The person has hypotonic dehydration, so give a hypertonic solution. • He has excess solute loss from GI distress, while replacing it with plain water. His plasma fluid has more water than particles, water moves from the plasma to the interstitial space, and then into the cells. This can lead to shock. • The headache is from the brain cells swelling from the excess water they have absorbed. • He should have replaced the electrolytes by drinking something like Gaitoraid or Pedialite.
Patient Case 3 • A 35 year old patient recovering from food poisoning has been vomiting and eating only Saltine crackers. • She has a moderately rapid pulse and moderately low blood pressure • Do you give an iv solution that is hyper, hypo, or isotonic? Why?
Patient Case 3 • She has a hypertonic fluid deficit, so she needs a hypotonic solution. • The salty crackers replaced the sodium lost from GI distress, but the salt replacement exceeded the water replacement, so her plasma is hypertonic.
Body Weight in Water • There are 100 trillion cells in your body, 25% of them are red blood cells (RBC’s). Dead RBCs are the reason why your pee is yellow and your poop is brown! You will understand why, later in the semester. • About 60% of your body weight is from water. How can you calculate your water weight? For every 2.2 pounds, you are 1 kg in weight. Take your weight in pounds and divide by 2.2. Then multiply that number by 0.6 to see how much water is in your body. • Water makes up 60% of our body weight • 70 kg man X 0.6 = 42 kg = 42 L of water is in his body • How much of your own weight is water? If you weigh 150 lbs: 150 lbs/ 2.2 = 68 kg 68 x 0.6 = 40.8 Liters
Body Fluid Compartments • The total amount of water in your body is divided into two compartments • Intracellular water is inside of your cells. Most of your water is here (60%). • Extracellular water is outside of your cells. There are three types. • Interstitial fluid (the water immediately outside cells, between and around cells) (30%) • Plasma fluid (the water inside blood vessels, but not in blood cells) (9%) • Transcellular fluid (the water enclosed in chambers lined by epithelial membranes, including the GI tract and synovial joints) (1%)
Composition of Compartments • All compartments are not the same size. Which is the biggest? Intracellular • What’s the smallest? Trancellular • The inside of each cell is low sodium and calcium, and high in potassium and proteins (there are four times as many proteins in cells than there are in plasma). • Outside of cells (in the plasma) are high in sodium and calcium, low in potassium and proteins. • Sodium has the highest extracellular fluid to intracellular fluid concentration ratio for most mammalian cells.
Homeostasis of Osmolarity • As stated, if you could count all the solutes (particles) inside and outside of the cell, they arethe same number (300 mOsm). Why does it need to be that way? • All particles pull water to them, whether the particle is glucose, calcium, a protein, salt, etc. We don’t want a net gain or loss of fluid across the cell membrane or the cell will shrink or burst. Not all compartments have the same volume liquid, but they all have the same number of particles per liter.
Cell membranes are semi-permeable • If the numbers of particles are always the same, how can we have higher numbers of potassium ions inside of the cell compared to the outside of the cell? • Won’t the potassium ions want to move down their concentration gradient towards equilibrium? • Yes, they will want to, but the cell membranes are designed to be semi-permeable (they will only let certain substances come into and go out of the cell). The cell membranes prevent potassium (and other particles) from crossing.
Diffusion • If you have a cell immersed in pure water, will it shrink or burst? • The particle concentration is higher in the cell than in pure water, so the particles want to leave the cell and enter the pure water. • However, they cannot do that because they are blocked in by the cell membrane. • That means there are more particles on the inside of the cell than in the pure water. Particles suck, so pure water will get sucked into the cell until the cell bursts. • In theory, if the substance we are talking about was a particle that can cross the cell membrane whenever it wants to, it would simply diffuse across the cell membrane until it reached equilibrium, so the cell would not burst.
What particles can cross the cell membrane? Gases (O2, CO2) Lipids and lipid-loving (hydrophobic or lipophilic) substances, such as alcohol
Functions of Membrane- Selective Permeability and Transport • Selectively permeable- allows some substances to pass between intracellular and extracellular fluids • Only small uncharged molecules or fat soluble molecules can pass through membrane without help. They get through by one of two types of ways: Passive transport means that energy (ATP) is not needed to get a particular substance across the cell membrane. Active transport means that ATP is used.
Membrane Function There are three types of Passive Transport: 1) Simple Diffusion 2) Facilitated Diffusion 3) Osmosis All of these involve particles crossing from high to low concentration. Osmosis is diffusion of WATER across a CELL MEMBRANE. Osmosis only happens if the solute is permeable across the cell membrane! http://www.northland.cc.mn.us/biology/BIOLOGY1111/animations/passive1.swf
Permeability • A water-hating (hydrophobic) substance can cross a cell membrane. • A very small water-loving (hydrophilic)substance can also cross, such as gasses or a water molecule itself. • However, a larger water-loving molecule needs a special protein channel in the cell membrane to help it to cross. • If it does not require energy (ATP), it is called facilitated diffusion (facilitated means “helping”). • If it requires ATP, it is crossing by an active transport mechanism.
Facilitated diffusion • Facilitated diffusion is when an ion wants to travel down its concentration gradient, but there is a channel in the cell membrane that opens and closes by a protein which enlarges or shrinks to open or block the channel (remember, this is still passive transport, so it does not need ATP).
Three types of Passive Transport: • Simple Diffusion • Facilitated Diffusion • Osmosis
Active Transport • Active Transport is when a substance needs to move against its concentration gradient (it is moved from an area of low concentration on one side of the cell membrane to an area of high concentration on the other side of the cell membrane). • It accomplishes this because a protein embedded in the cell membrane grabs onto the substance and drags it across the cell membrane (this requires ATP).
Active Transport • There are three main types of active transport: • Ion Pumps • Cotransport • Endocytosis • Because these are active transport mechanisms, ATP is used. http://www.northland.cc.mn.us/biology/BIOLOGY1111/animations/active1.swf
Transport of Water • There are two ways that water can move: • Osmosis • Hydrostatic pressure
Movement of water • Always passive • Pores (called aquaporins) in the cell membrane serve as conduits (conducting channel) • Osmosis • Water wants to move from its area of high concentration (less particles in the water) to its area of low concentration (more particles in the water). When it crosses a cell membrane to do this, it is called osmosis. • In a solution, water is called the solvent and the particles are called the solutes. • Hydrostatic pressure • This is the pressure of the fluid exerted on the vessels, or container. If you squeezed on this bottle to get the water to shoot out, what kind of pressure would this simulate?
Hydrostatic Pressure • Squeeze a water bottle to shoot the water out, this is hydrostatic pressure. Hydrostatic pressure is the pressure of the water exerting on the blood vessel wall. If you push harder, the water will shoot farther. • The hydrostatic pressure of water being filled in a balloon will exceed the capacity of the balloon and pop. • That is how water moves between cells and into cells so that plasma becomes interstitial fluid. The plasma leaks out between the cells that make up the capillaries. • If you have a swollen ankle and apply an ace wrap, you are applying hydrostatic pressure to force interstitial fluid back into the plasma. Hydrostatic pressure is not the movement across a cell membrane. That is osmosis.
Osmosis • Osmosis is movement of water across the cell membrane. Osmosis will occur when there is a difference of particle concentration on each side of a cell membrane. • Osmotic pressure can be measured. If there is more water on one side of a membrane than the other side of the membrane, the water will move down its concentration gradient. This occurs when there are more particles on one side of the membrane than the other, but the particles are not free to diffuse across until they reach equilibrium.
Dialysis Tubing Demonstration • Dialysis tubing is a flexible tube that looks like plastic sausage tubes, but they are semipermeable like a real cell membrane. Dialysis tubing is used in laboratory demonstrations about osmosis because it is not permeable to glucose but water can cross it. • It helps you learn about the body because glucose also cannot get across the body’s cell membranes, but water can.
In another laboratory demonstration, water will move past a sheet of dialysis tubing in a column until it reaches a certain column height. • It does not continue to climb higher and higher in the column indefinitely, because gravity will be exerting forces on it too (hydrostatic pressure). • Eventually, the water will reach a certain height and then stop.