Download
1 / 47
530 likes | 1.7k Views
Hypoxic-Ischemic Encephalopathy (HIE). Dezhi Mu MD/PhD Department of Pediatrics/Children’s Medical Center West China Second University Hospital, Sichuan University. Contents. 1. Etiology. 2. Pathophysiology. 3. Clinical manifestations. 4. Laboratory tests. 5. Treatment. Definition.

E N D
Hypoxic-Ischemic Encephalopathy (HIE) Dezhi Mu MD/PhD Department of Pediatrics/Children’s Medical Center West China Second University Hospital, Sichuan University
Contents 1.Etiology 2. Pathophysiology 3. Clinical manifestations 4. Laboratory tests 5. Treatment
Definition Incidence: 3~9 per 1000 live births Hypoxia: PaO2↓ HIE + Ischemia: Blood flow↓
Etiology 1. Maternal Causes 2. Placental / Unbilical Causes HIE 3. Neonatal Causes
Etiology • Maternal Causes 1. Reduced maternal oxygen delivery Anemia Cardiovascular disease Hypotension/hypertension 2. Reduced uterine blood flow Abnormal uterine contractions
Etiology Placenta Umbilical vein Umbilical arteries • Placental Causes 1. Early placental separation 2. Placental dysfunction Prematurity、Postmaturity Placentitis Placental edema
Etiology Placenta Umbilical vein umbilical cord Umbilical arteries Umbilical Causes Reduced umbilical blood flow Excessive length of umbilical cord Short of umbilical cord Knots of umbilical cord
Etiology Neonatal Causes 1. Preterm、Low birth weight、SGA、LGA 2. Diseases Asphxia、Septicemia Pulmonary disease Congenital cardiovascular disease
Pathophysiology Hypoxemia Brain hypoxia and ischemia Reperfusion injury Depleting ATP: energy failure Secondaryenergy failure Primary cell death (necrotic) Secondary cell death (apoptotic) 6 h 6~24h HIE
Clinical Manifestations Mild Depending on HIE severity Moderate Severe
Accessory tests- laboratory test No specific test to confirm the diagnosis. Tests are performed to assess the injury and to monitor functional status of the organs.
Accessory tests • Electroencephalogram (EEG) 1. Assess the severity of the injury 2. Evaluate for subclinical seizures 3. A suppressed or seizure activity of EEG A poor prognosis
Accessory tests • Cranial Computed tomograph scan 1、Cerebral edema 2、Hemorrhage Potentially harmful radiation
Accessory tests Cerebral edema Normal CT: Cerebral edema
Accessory tests Normal Hemorrhage CT
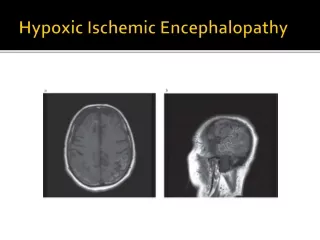
Accessory tests • Brain MRI 1、Accurately demonstrate the injury pattern as area of hyperintensity 2、Diagnosis and follow-up of infants with moderate-to-severe HIE
Accessory tests Cerebral edema Normal MRI: Cerebral edema
Accessory tests Hypoperfusion injury Normal Hypoperfusion injury;signal intensity
Treatments Supportive treatment Specific treatment: N/A Recovery treatment
Treatments Management aims at: 1. Early identification 2. To maintain adequate perfusion 3. To stop the processes of ongoing injury
Treatments • Therapeutic Window 1. Clinic: No direct evidence 2. Studies: Animal models 3. When: 6h
Treatments Supportive treatments 1. Adequate ventilation 2. Adequate perfusion 3. Adequate Glucose
Treatments Adequate ventilation 80mmHg<PaO2<100mmHg 20mmHg<PaCO2<40mmHg pH: 7.35~7.45
Treatments Supportive care 1. Adequate ventilation 2. Adequate perfusion 3. Adequate Glucose
Treatments • Adequate perfusion • Peripheral perfusion • Blood pressure: 70/50 mmHg • Echocardiography (ECHO) Fluids: 60~80 mL/kg .d Dopamine: 2.5~5μg/kg. min
Treatments Supportive care 1. Adequate ventilation 2. Adequate perfusion 3. Adequate glucose
Treatments Aim: Avoidance of hypoglycemia/hyperglycemia Maintain the glucose: 40~90mg/dl Maintain the normal electrolytes
Treatments Symptomatic treatment 1. Treatment of seizures 2. Treatment of intracranial pressure
Treatments Neonatal seizures 1. HIE is the most common cause of seizures 2. About 30% of HIE at the first 24 hours 3. Increase the risk of additional injury
Treatments • Treatment of seizures Drug: Phenobarbitone (first line treatment) 20 mg/kg, intravenously repeated once as needed daily dosing 5 mg/kg/day (target level 40–60 g/mL)
Treatments Symptomatic treatment 1. Treatment of seizures 2. Treatment of intracranial pressure
Treatments • Treatment of intracranial pressure • Fluids: 60~80 mL/kg .d • Furosemide ? • Mannitol ?
Treatments Current potential treatment Hypothermia
Treatments • Hypothermia is used for the following: • ≥ 35 weeks gestational age • ≥ 1800g • moderate to severe encephalopathy • intrapartum hypoxia indicated as following: (1) Apgar score ≤ 5 at 10 minutes (2) blood gas with pH ≤ 7.00
Treatments • Optimal timing of initiation • Within 6 hours, the earlier the better • Temperature • 3~4℃ below baseline temperature, 33.0~34.0℃ • Optimal duration • 72h, the greater severity, the longer • Methods • Selective head / Whole body cooling
Prognosis Death: 15~20% in neonatal period Neurodevelopmental abnormalities: 25~30% survivors Mild: recover completely Moderate: about 20% neurological complications Severe: most die or severe brain injury
Case discussion Male infant, 30 minutes. Complaint: Poor response after resuscitation for 30 minutes, convulsed once. History: Born by emergency CS for suspected fetal distress. Apgar score: 0, 0, 2 at 1, 5, 10minutes. Meconium-staining of amniotic fluid.
To be continued No breath and heart beat at birth, intubated in the delivery room. Hypotonia and pale skin were noted. Face-masked pressure respiration, chest compression and epinephrine were used. 10 minutes after resuscitation, his eyes starred for about 1 minute.
To be continued PE: Poor response, cyanotic lips. Normal anterior fontanelle tension. Muscular tension was low. Primary reflections could not be elicited.
To be continued Investigation: Chest X-ray: neonate pneumonia. Blood gas analysis: pH 6.948,SaO2 82%, HCO3- 11mmol/L. Liver and kidney function, blood electrolytes, Blood-Rt, CRP: normality
Case discussion continued Question: 1. What is the diagnosis? 2. What is the investigation? 3. What is the treatment?
Case discussion continued Diagnosis: 1. Hypoxic ischemic encephalopathy (severe) 2. Neonatal asphyxia (severe)
Case discussion continued Investigation: 1. Brain CT and MRI: decreased density of intracranial cerebral white matter; the left frontal top soft tissue swelling. 2. EEG: abnormal, a spike or wide sharp wave repeatedly issuing.
Case discussion continued Treatment: 1. supportive treatment. 2. hypothermia 3. rehabilitation
Thank you! mudz@scu.edu.cn • 028-85501313(O)