Download
1 / 1
30 likes | 228 Views
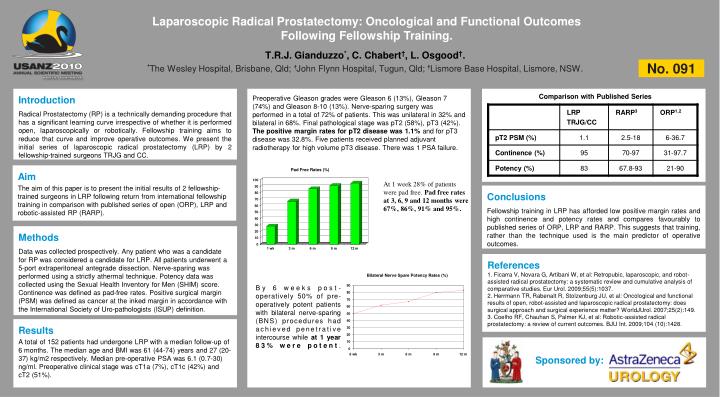
Laparoscopic Radical Prostatectomy: Oncological and Functional Outcomes Following Fellowship Training. T.R.J. Gianduzzo * , C. Chabert † , L. Osgood † . * The Wesley Hospital, Brisbane, Qld; † John Flynn Hospital, Tugun, Qld; † Lismore Base Hospital, Lismore, NSW. No. 091.

E N D
Laparoscopic Radical Prostatectomy: Oncological and Functional Outcomes Following Fellowship Training. T.R.J. Gianduzzo*, C. Chabert†, L. Osgood†. *The Wesley Hospital, Brisbane, Qld; †John Flynn Hospital, Tugun, Qld; †Lismore Base Hospital, Lismore, NSW. No. 091 Comparison with Published Series Introduction Radical Prostatectomy (RP) is a technically demanding procedure that has a significant learning curve irrespective of whether it is performed open, laparoscopically or robotically. Fellowship training aims to reduce that curve and improve operative outcomes. We present the initial series of laparoscopic radical prostatectomy (LRP) by 2 fellowship-trained surgeons TRJG and CC. Preoperative Gleason grades were Gleason 6 (13%), Gleason 7 (74%) and Gleason 8-10 (13%). Nerve-sparing surgery was performed in a total of 72% of patients. This was unilateral in 32% and bilateral in 68%. Final pathological stage was pT2 (58%), pT3 (42%). The positive margin rates for pT2 disease was 1.1% and for pT3 disease was 32.8%. Five patients received planned adjuvant radiotherapy for high volume pT3 disease. There was 1 PSA failure. Aim The aim of this paper is to present the initial results of 2 fellowship-trained surgeons in LRP following return from international fellowship training in comparison with published series of open (ORP), LRP and robotic-assisted RP (RARP). At 1 week 28% of patients were pad free. Pad free rates at 3, 6, 9 and 12 months were 67%, 86%, 91% and 95%. Conclusions Fellowship training in LRP has afforded low positive margin rates and high continence and potency rates and compares favourably to published series of ORP, LRP and RARP. This suggests that training, rather than the technique used is the main predictor of operative outcomes. Methods Data was collected prospectively. Any patient who was a candidate for RP was considered a candidate for LRP. All patients underwent a 5-port extraperitoneal antegrade dissection. Nerve-sparing was performed using a strictly athermal technique. Potency data was collected using the Sexual Health Inventory for Men (SHIM) score. Continence was defined as pad-free rates. Positive surgical margin (PSM) was defined as cancer at the inked margin in accordance with the International Society of Uro-pathologists (ISUP) definition. References 1. Ficarra V, Novara G, Artibani W, et al: Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol. 2009;55(5):1037. 2. Herrmann TR, Rabenalt R, Stolzenburg JU, et al: Oncological and functional results of open, robot-assisted and laparoscopic radical prostatectomy: does surgical approach and surgical experience matter? WorldJUrol. 2007;25(2):149. 3. Coelho RF, Chauhan S, Palmer KJ, et al: Robotic-assisted radical prostatectomy: a review of current outcomes. BJU Int. 2009;104 (10):1428. By 6 weeks post-operatively 50% of pre-operatively potent patients with bilateral nerve-sparing (BNS) procedures had achieved penetrative intercourse while at 1 year 83% were potent. Results A total of 152 patients had undergone LRP with a median follow-up of 6 months. The median age and BMI was 61 (44-74) years and 27 (20-37) kg/m2 respectively. Median pre-operative PSA was 6.1 (0.7-30) ng/ml. Preoperative clinical stage was cT1a (7%), cT1c (42%) and cT2 (51%). Sponsoredby: