Download
1 / 1
10 likes | 242 Views
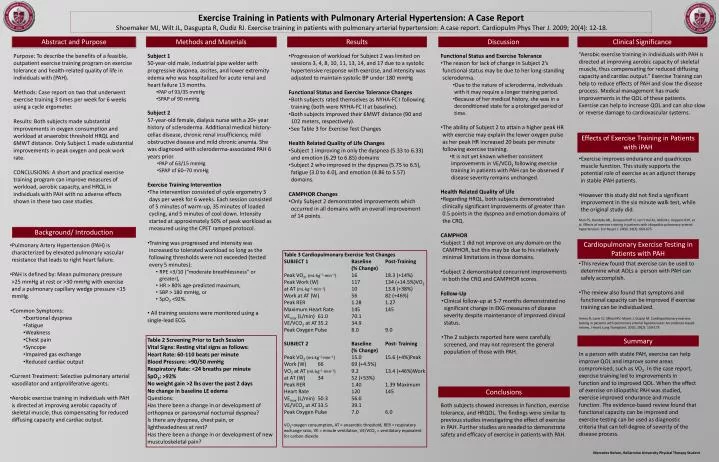
Exercise Training in Patients with Pulmonary Arterial Hypertension: A Case Report Shoemaker MJ, Wilt JL, Dasgupta R, Oudiz RJ. Exercise training in patients with pulmonary arterial hypertension: A case report. Cardiopulm Phys Ther J. 2009; 20(4): 12-18. Abstract and Purpose.

E N D
Exercise Training in Patients with Pulmonary Arterial Hypertension: A Case Report Shoemaker MJ, Wilt JL, Dasgupta R, Oudiz RJ. Exercise training in patients with pulmonary arterial hypertension: A case report. Cardiopulm Phys Ther J. 2009; 20(4): 12-18. Abstract and Purpose Methods and Materials Results Discussion Clinical Significance “Aerobic exercise training in individuals with PAH is directed at improving aerobic capacity of skeletal muscle, thus compensating for reduced diffusing capacity and cardiac output.” Exercise Training can help to reduce effects of PAH and slow the disease process. Medical management has made improvements in the QOL of these patients. Exercise can help to increase QOL and can also slow or reverse damage to cardiovascular systems. Purpose: To describe the benefits of a feasible, outpatient exercise training program on exercise tolerance and health-related quality of life in individuals with (PAH). Methods: Case report on two that underwent exercise training 3 times per week for 6 weeks using a cycle ergometer. Results: Both subjects made substantial improvements in oxygen consumption and workload at anaerobic threshold HRQL and 6MWT distance. Only Subject 1 made substantial improvements in peak oxygen and peak work rate. CONCLUSIONS: A short and practical exercise training program can improve measures of workload, aerobic capacity, and HRQL in individuals with PAH with no adverse effects shown in these two case studies. • Subject 1 • 50-year-old male, industrial pipe welder with progressive dyspnea, ascites, and lower extremity edema who was hospitalized for acute renal and heart failure 13 months. • PAP of 93/35 mmHg • SPAP of 90 mmHg • Subject 2 • 57-year-old female, dialysis nurse with a 20+ year history of scleroderma. Additional medical history- celiac disease, chronic renal insufficiency, mild obstructive disease and mild chronic anemia. She was diagnosed with scleroderma-associated PAH 6 years prior. • PAP of 63/15 mmHg • SPAP of 60–70 mmHg • Exercise Training Intervention • The intervention consisted of cycle ergometry 3 days per week for 6 weeks. Each session consisted of 5 minutes of warm-up, 35 minutes of loaded cycling, and 5 minutes of cool down. Intensity started at approximately 50% of peak workload as measured using the CPET ramped protocol. • Training was progressed and intensity was increased to tolerated workload so long as the following thresholds were not exceeded (tested every 5 minutes): • RPE >3/10 (“moderate breathlessness” or greater), • HR > 80% age-predicted maximum, • SBP > 180 mmHg, or • SpO2 <92%. • All training sessions were monitored using a single-lead ECG. • Progression of workload for Subject 2 was limited on sessions 3, 4, 8, 10, 11, 13, 14, and 17 due to a systolic hypertensive response with exercise, and intensity was adjusted to maintain systolic BP under 180 mmHg • Functional Status and Exercise Tolerance Changes • Both subjects rated themselves as NYHA-FC I following training (both were NYHA-FC II at baseline). • Both subjects improved their 6MWT distance (90 and 102 meters, respectively). • See Table 3 for Exercise Test Changes • Health Related Quality of Life Changes • Subject 1 improving in only the dyspnea (5.33 to 6.33) and emotion (6.29 to 6.85) domains • Subject 2 who improved in the dyspnea (5.75 to 6.5), fatigue (3.0 to 4.0), and emotion (4.86 to 5.57) domains. • CAMPHOR Changes • Only Subject 2 demonstrated improvements which occurred in all domains with an overall improvement of 14 points. • Functional Status and Exercise Tolerance • The reason for lack of change in Subject 2’s functional status may be due to her long-standing scleroderma. • Due to the nature of scleroderma, individuals with it may require a longer training period. • Because of her medical history, she was in a deconditioned state for a prolonged period of time. • The ability of Subject 2 to attain a higher peak HR with exercise may explain the lower oxygen pulse as her peak HR increased 20 beats per minute following exercise training. • It is not yet known whether consistent improvements in VE/VCO2 following exercise training in patients with PAH can be observed if disease severity remains unchanged. • Health Related Quality of Life • Regarding HRQL, both subjects demonstrated clinically significant improvements of greater than 0.5 points in the dyspnea and emotion domains of the CRQ. • CAMPHOR • Subject 1 did not improve on any domain on the CAMPHOR, but this may be due to his relatively minimal limitations in those domains. • Subject 2 demonstrated concurrent improvements in both the CRQ and CAMPHOR scores. • Follow-Up • Clinical follow-up at 5-7 months demonstrated no significant change in EKG measures of disease severity despite maintenance of improved clinical status. • The 2 subjects reported here were carefully screened, and may not represent the general population of those with PAH. Effects of Exercise Training in Patients with iPAH • Exercise improves endurance and quadriceps muscle function. This study supports the potential role of exercise as an adjunct therapy in stable iPAH patients. • However this study did not find a significant improvement in the six minute walk test, while the original study did. • Man FS, Handoko ML, Groepenhoff H, van’t Hul AJ, Abbink J, Koppers RJH, et al. Effects of exercise training in patients with idiopathic pulmonary arterial hypertension. Eur Respir J. 2009; 34(3): 669-675 Background/ Introduction Cardiopulmonary Exercise Testing in Patients with PAH • Pulmonary Artery Hypertension (PAH) is characterized by elevated pulmonary vascular resistance that leads to right heart failure. • PAH is defined by: Mean pulmonary pressure >25 mmHg at rest or >30 mmHg with exercise and a pulmonary capillary wedge pressure <15 mmHg. • Common Symptoms: • Exertional dyspnea • Fatigue • Weakness • Chest pain • Syncope • Impaired gas exchange • Reduced cardiac output • Current Treatment: Selective pulmonary arterial vasodilator and antiproliferative agents. • Aerobic exercise training in individuals with PAH is directed at improving aerobic capacity of skeletal muscle, thus compensating for reduced diffusing capacity and cardiac output. Table 3 Cardiopulmonary Exercise Test Changes SUBJECT 1 BaselinePost-Training (% Change) Peak VO2, (mL·kg−1·min−1) 16 18.3 (+14%) Peak Work (W) 117 134 (+14.5%)VO2at AT (mL·kg−1·min−1) 10 13.8 (+38%) Work at AT (W) 56 82 (+46%) Peak RER 1.28 1.27 Maximum Heart Rate 145 145 VEmax(L/min) 61.0 70.1 VE/VCO2 at AT 35.2 34.9 Peak Oxygen Pulse 8.0 9.0 SUBJECT 2 Baseline Post- Training (% Change) Peak VO2(mL·kg−1·min−1) 15.0 15.6 (+4%)Peak Work (W) 66 69 (+4.5%) VO2at AT (mL·kg−1·min−1) 9.2 13.4 (+46%)Work at AT (W) 34 52 (+53%) Peak RER 1.401.39 Maximum Heart Rate 120145 VEmax(L/min) 50.356.0 VE/VCO2 at AT 33.539.1 Peak Oxygen Pulse 7.0 6.0 VO2=oxygen consumption, AT = anaerobic threshold, RER = respiratory exchange ratio, VE = minute ventilation, VE/VCO2 = ventilatory equivalent for carbon dioxide • This review found that exercise can be used to determine what ADLs a person with PAH can safely accomplish. • The review also found that symptoms and functional capacity can be improved if exercise training can be individualized. • Arena R, Lavie CJ, Milani RV, Myers J, Guazzi M. Cardiopulmonary exercise testing in patients with pulmonary arterial hypertension: An evidence-based review. J Heart Lung Transplant. 2010; 29(2): 159-173 Table 2 Screening Prior to Each Session Vital Signs: Resting vital signs as follows: Heart Rate: 60-110 beats per minute Blood Pressure: >90/50 mmHg Respiratory Rate: <24 breaths per minute SpO2: >92% No weight gain >2 lbs over the past 2 days No change in baseline LE edema Questions: Has there been a change in or development of orthopnea or paroxysmal nocturnal dyspnea? Is there any dyspnea, chest pain, or lightheadedness at rest? Has there been a change in or development of new musculoskeletal pain? Summary In a person with stable PAH, exercise can help improve QOL and improve some areas compromised, such as VO2. In the case report, exercise training led to improvements in function and to improved QOL. When the effect of exercise on idiopathic PAH was studied, exercise improved endurance and muscle function. The evidence-based review found that functional capacity can be improved and exercise testing can be used as diagnostic criteria that can tell degree of severity of the disease process. Conclusions Both subjectsshowed increasesin function, exercise tolerance, and HRQOL. The findings were similar to previous studies investigating the effect of exercise in PAH. Further studiesare needed to demonstrate safety and efficacy of exercise in patients with PAH. Mercedes Nelson, Bellarmine University Physical Therapy Student