Download

1 / 37
370 likes | 467 Views
Hypersensitivity محمد فهد المسعود 431102617 عاصم فهد الدهيش 430106507 عوض عبدالله الحربي 431102322. Introduction.

E N D
Hypersensitivity محمد فهد المسعود 431102617 عاصم فهد الدهيش 430106507 عوض عبداللهالحربي 431102322
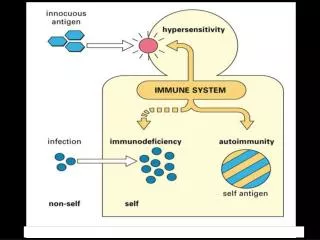
Introduction the immune response uses multiple strategies to reduce damage to self by turning off responses when pathogen is cleared and avoiding reactions to self antigens. However, these checks and balances can break down, leading to immune-mediated reactions that are more detrimental than protective.
Introduction What is the Hypersensitivity ? Hypersensitivity refers to excessive, reactions produced by the normal immune system. Hypersensitivity reactions are harmful antigen-specific immune responses , occur when an individual who has been primed by an innocuous antigen subsequently encounters the same antigen , produce tissue injury and dysfuntion
Hypersensitivityreactions • Hypersensitivity reactions can be divided into four types: type I, type II, type III and type IV, based on the mechanisms involved and time taken for the reaction. Frequently, a particular clinical condition (disease) may involve more than one type of reaction.
TYPE I Hypersensitivity OR (IgE-mediated) is also known as immediate or anaphylactic hypersensitivity. The reaction may involve skin (urticaria and eczema), eyes (conjunctivitis), nasopharynx (rhinorrhea, rhinitis), bronchopulmonary tissues (asthma) and gastrointestinal tract (gastroenteritis). The reaction may cause a range of symptoms from minor inconvenience to death. The reaction usually takes 15 - 30 minutes from the time of exposure to the antigen.
TYPE IHypersensitivity Immediate hypersensitivity is mediated by IgE. The primary cellular component in this hypersensitivity is the mast cell or basophil. Healthy individuals generate IgE antibodies only in response to parasitic infections. However, some people referred to as atopic , are predisposed to generate IgE antibodies against common environmental antigens (Plant pollens – Foods- Drugs- Insect products).
Type I reactions occur in two phases - Sensitization phase First contact with allergens - Challenge phase Subsequent contact with allergens
Normal nose Allergy: Rhinitis, Eczema & Conjunctivitis
TYPE II Hypersensitivity is also known as ( cytotoxic hypersensitivity). the antibodies (IgM & IgG) produced by the immune response bind to antigens on the patient's own cell surfaces (antibody-mediated). Antibody bound to a cell-surface antigen can induce death of the antibody-bound cell
Mechanism of killing targeted cells : 1) Certain immunoglobulin subclasses can activate the complement system. 2) antibodies can mediate cell destruction by antibody dependent cell-mediated cytotoxicity (ADCC), in which cytotoxic cells bearing Fc receptors bind to the Fc region of antibodies on target cells and promote killing of the cells. 3) antibody bound to a foreign cell also can serve as an opsonin. (molecule that enhances phagocytosis by marking an antigen for an immune response)
Transfusion Reactions Transfusion reactions are an example of type II hypersensitivity, on the membrane of red blood cells are encoded by genes with several allelic forms. An individual with a particular allele of a blood-group antigen can recognize other allelic forms in transfused blood as foreign. Blood types are referred to as A, B, or O, and the antigens that are associated with the blood types are identified as A, B, and H.
Transfusion Reactions When the antibodies directed toward ABH antigens are termed Isohemagglutinins For example, If a type A individual is transfused with blood containing type B cells, a transfusion reaction occurs in which the preexisting anti-B isohemagglutinins bind to the B blood cells and mediate their destruction by means of complement-mediated lysis. Individuals with blood type O express only the H antigen. Although they can donate blood to anyone.
Hemolytic Disease of the Newborn Hemolytic disease of the newborn develops when maternal IgG antibodies specific for fetal blood-group antigens cross the placenta and destroy fetal red blood cells. An Rh- mother fertilized by an Rh+ father is in danger of developing a response to the Rh antigen and rejecting an Rh+ fetus. at the time of delivery, separation of the placenta from the uterine wall allows larger amounts of fetal umbilical cord blood to enter the mother’s circulation. These fetal red blood cells stimulate Rh-specific B cells to mount an immune response.
Hemolytic Disease of the Newborn • Hemolytic disease of the newborn caused by Rh incompatibility in a second or later pregnancy can be almost entirely prevented by administering antibodies against the Rh antigen to the mother at around 28 weeks of pregnancy and within 24 to 48 hours after the first delivery.
TYPE III hypersensitivity reaction • Phase 1 • Immune complex formation • IgM and IgGbind to soluble Ag whichlead to immune comlex formation • Soluble Ag-Ab complexthat are large in size are clearedfrom circulation by phagocyte cell (liver and spleen)
Phase 2 Immune complex deposition They are deposited in capillary walls either: • Locally at site Ag entry • Systematically in blood vessels and various tissue Phase 3 Immune complex-mediated inflamation Ag-Ab complex stimulate complement activation causing tissue damage
-Factors that determine whether immune complex formation will lead to tissue deposition and disease are Size of immune complexes and functional status of the mononuclear phagocyte system 1) large complexes in antibody or excess are rapidly removed from circulation by mononuclear phagocyte system (harmless) 2)Pathogenic complexes are small or intermediate, which bind less avidly to phagocytic cells circulate longer
Immune complex-mediated diseases can be 1)generalized immune complexes are formed in circulation and deposited in many organs 2)localized deposited to particular organs, such as kidney (glomerulonephritis), joints (arthritis), or small blood vessels.
Two types of antigens cause immune complex –mediated injury : 1) Antigen may be exogenous (foreign protein, bacterium, or virus) 2) Individual can produce antibody against self-components (endogenous antigens); antigen compounds of one’s own cells/tissues such as nuclear antigens, immunoglobulin or tumour antigens.
Systemic Immune Complex Disease serum sickness - patients with diphtheria infection treated with serum from horses immunized with diphtheria toxin - patients develop arthritis, skin rash, fever - patients made antibodies to horse serum proteins antibodies formed complexes with injected proteins, and disease was due to antibodies or immune complexes
Type IV hypersensitivity Mediated by T cells rather than by antibodies. Two types of reactions mediated by different T cells subsets : 1. Delayed type hypersensitivity initiated by CD 4 T cells 2. Cellular cytotoxicity, mediated by CD 8 + T cells
-In both cases, the reaction is initiated by exposure of sensitized T cells to specific antigenic peptides bound to self-MHC molecules, but the subsequent events are different. -In delayed Hypersensitivity Type4 type CD4+ T Cells secrete cytokines, leading to recruitment of other cells, especially macrophages, which are the major effector cells. -In cell mediated cytotoxicity, cytotoxic CD8+ T cells themselves assume the effector function
Three types of DTH 1. Contact Hypersensitivity2. Tuberculin type Hypersensitivity. • Both occur within 72 hours of antigen challenge3. Granulomatous Hypersensitivity • Develop over a period of 21-28 days. • Formed by the aggregation and proliferation of macrophages and may persist for weeks. • Most serious type of type IV hypersensitivity response
1-Contact Hypersensitivity • Characterized by a reaction at the site of contact with the allergen (eg. Contact Hypersensitivity ). • Caused by haptense.gnickle, chemical in rubber, cosmatics, hair dye • The cell involved in antigen presentation at this site is the langerhans cell. The pathway from initial exposure involves sensitization (with Langerhans cells presenting Ag to CD4+ helper T-cells) and exposure , followed by aggregation of mononuclear cells around blood vessels and glands in the epidermis and edema. A variety of cytokines are involved in this process, including IL-2, IL-3, IFN and GM-CSF. The reaction decreases 48-72 hours following exposure
Sensitization phase Haptens penetrate epidermis Haptens conjugated to body proteins Complex internalized by langerhans cell (APC) APC migrated to regional lymph nodes APC present Ag to CD4+ cells (TDTH)
Effector phase Up on 2nd exposure, Skin become infiltrated With activated. TDTH (CD4+Th1) and few CD8+, MQ, cytokines release Eczematous reaction is seen locally in 48-72 hs (swelling and erythema)
3- Granulomatous Hypersensitivity This type of reaction is characterized by persistance of the antigen within macrophages as well as of the lesion. Such antigens are particulate matter such as talc and silica but also mycobacteria. The characteristic cells found in the lesion are epitheloid cells (probably macrophages) and giant-cells (multi-nucleated macrophages). The granuloma consists of a hard core of cells sometimes with a necrotic core. This is surrounded by lymphocytes with a deposition of collagen fibres.