Download
1 / 64
640 likes | 797 Views
The Prevalence, Co-morbidity, and Treatment of Mental Health, Substance, and Crime Problems among Teenagers. Michael Dennis, Ph.D. Chestnut Health Systems, Bloomington, IL

E N D
The Prevalence, Co-morbidity, and Treatment of Mental Health, Substance, and Crime Problems among Teenagers Michael Dennis, Ph.D. Chestnut Health Systems, Bloomington, IL Presentation at “Pediatric Mental Health Primer V: The Complex Needs of Children with Dual Diagnosis (Mental Illness and Substance Abuse)”, September 18, 2007, InPlay’s Forté Conference Center, Peoria, IL. The content of this presentations are based on treatment & research funded by the Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA) under contract 270-2003-00006 and several individual grants. The opinions are those of the author and do not reflect official positions of the consortium or government. Available on line at www.chestnut.org/LI/Posters or by contacting Joan Unsicker at 720 West Chestnut, Bloomington, IL 61701, phone: (309) 827-6026, fax: (309) 829-4661, e-Mail: junsicker@Chestnut.Org
Goals of this Presentation • To examine the prevalence, course, and consequences of adolescent substance use and co-occurring disorders and the unmet need for treatment • To summarize major trends, variability and problems in the adolescent treatment system • To present the findings from several recent treatment outcome studies on substance abuse treatment research, trauma and violence/crime.
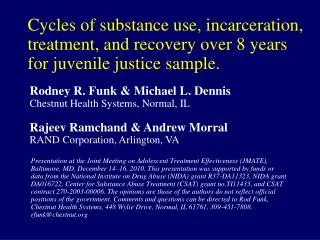
Adolescent Onset Remission Severity of Past Year Substance Use/Disorders by Age NSDUH Age Groups Increasing rate of non-users 100 Severity Category 90 No Alcohol or Drug Use 80 70 Light Alcohol Use Only 60 Any Infrequent Drug Use 50 40 Regular AOD Use 30 Abuse 20 10 Dependence 0 2002 U.S. Household Population age 12+ = 235,143,246 65+ 12-13 14-15 16-17 18-20 21-29 30-34 35-49 50-64 Source: 2002 NSDUH and Dennis & Scott in press
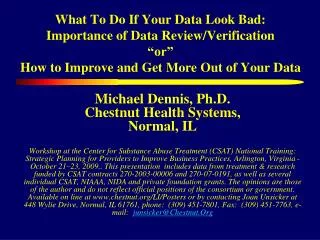
Mean (95% CI) $3,058 This includes people who are in recovery, elderly, or do not use because of health problems Higher Costs $1,613 $1,528 $1,309 $1,078 $948 Higher Severity is Associated with Higher Annual Cost to Society Per Person $4,000 Median (50th percentile) $3,500 $3,000 $2,500 $2,000 $1,500 $1,000 $725 $406 $500 $231 $231 $0 $0 $0 No Alcohol or Light Alcohol Regular AOD Any Dependence Abuse Infrequent Drug Use Use Only Drug Use Use Source: 2002 NSDUH
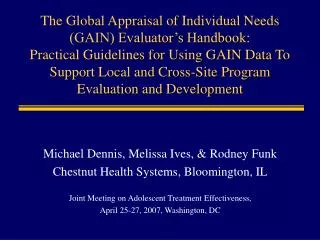
Substance Use Careers Last for Decades 1.0 Median of 27 years from first use to 1+ years abstinence .9 Cumulative Survival .8 .7 Years from first use to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Substance Use Careers are Longer the Younger the Age of First Use Age of 1st Use Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence .6 .5 under 15* .4 15-20* .3 .2 21+ .1 0.0 * p<.05 (different from 21+) 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Substance Use Careers are Shorter the Sooner People Get to Treatment Year to 1st Tx Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence 20+ .6 .5 .4 .3 10-19* .2 .1 0.0 0-9* * p<.05 (different from 20+) 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Treatment Careers Last for Years 1.0 .9 Cumulative Survival .8 Median of 3 to 4 episodes of treatment over 9 years .7 Years from first Tx to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25 Source: Dennis et al., 2005
Need for Treatment (% of 24,753,586 Adolescents in the U.S. Household Population) 10% 15% 20% 25% 0% 5% 14.9% Tobacco 17.8% Alcohol 10.7% Alcohol Binge --------Past Month Use------ 11.5% Any Drug Use 8.1% Marijuana Use Any Non-Marijuana Drug Use 5.7% Past Year AOD Dependence or Abuse 8.9% Less than 1 in 10 getting treatment Any Treatment (From NHSDA) 0.7% 88% of adolescents are treated in the public system Public Treatment (From TEDS) 0.6% Source: NSDUH and TEDS (see state level estimates in appendix)
Unmet Treatment Need Adolescent (% of AOD Dependence/Abuse without any private/public treatment) 9 in 10 Untreated Prevalence 82.4 to 90.1% 90.2 to 92.3% 92.4 to 94.2% 94.3 to 98.0% U.S.Avg.=92.2% IL=92.5% Source: Wright, D., & Sathe, N. (2005). State Estimates of Substance Use from the 2002–2003 National Surveys on Drug Use and Health (DHHS Publication No. SMA 05-3989, NSDUH Series H-26). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies (retrieved from http://oas.samhsa.gov/2k3State/2k3SAE.pdf )
64% increase from 95,271 in 1993 to 158,723 in 2005 Adolescent Treatment Admissions have increased by 61% over the past decade Source: Office of Applied Studies 1992- 2002 Treatment Episode Data Set (TEDS) http://www.samhsa.gov/oas/dasis.htm
Baseline Severity Goes up with Level of Care Detox: Higher on Use, but lower on prior tx Detox: Higher on Use Severity Goes up with Level of Care STR: Higher on Dependence 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Weekly use First used Prior Treatment Case Mix Index (Avg) Dependence at intake under age 15 Outpatient Intensive Outpatient Detoxification Long-term Residential Short-term Residential Source: Treatment Episode Data Set (TEDS) 1993-2003.
Median Length of Stay is only 50 days Median Length of Stay Total 50 days (61,153 discharges) Less than 25% stay the 90 days or longer time recommended by NIDA Researchers STR 21 days (5,152 discharges) LTR 49 days (5,476 discharges) Level of Care Detox 3 days (3,185 discharges) IOP 46 days (10,292 discharges) Outpatient 59 days (37,048 discharges) 0 30 60 90 Source: Data received through August 4, 2004 from 23 States (CA, CO, GA, HI, IA, IL, KS, MA, MD, ME, MI, MN, MO, MT, NE, NJ, OH, OK, RI, SC, TX, UT, WY) as reported in Office of Applied Studies (OAS; 2005). Treatment Episode Data Set (TEDS): 2002. Discharges from Substance Abuse Treatment Services, DASIS Series: S-25, DHHS Publication No. (SMA) 04-3967, Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from http://wwwdasis.samhsa.gov/teds02/2002_teds_rpt_d.pdf .
Despite being widely recommended, only 10% step down after intensive treatment 53% Have Unfavorable Discharges Total (61,153 discharges) STR (5,152 discharges) LTR (5,476 discharges) Detox (3,185 discharges) IOP (10,292 discharges) Outpatient (37,048 discharges) 0% 20% 40% 60% 80% 100% Completed Transferred ASA/ Drop out AD/Terminated Source: Data received through August 4, 2004 from 23 States (CA, CO, GA, HI, IA, IL, KS, MA, MD, ME, MI, MN, MO, MT, NE, NJ, OH, OK, RI, SC, TX, UT, WY) as reported in Office of Applied Studies (OAS; 2005). Treatment Episode Data Set (TEDS): 2002. Discharges from Substance Abuse Treatment Services, DASIS Series: S-25, DHHS Publication No. (SMA) 04-3967, Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from http://wwwdasis.samhsa.gov/teds02/2002_teds_rpt_d.pdf .
Most Lack of Standardized Assessment for… • Substance use disorders (e.g., abuse, dependence, withdrawal), readiness for change, relapse potential and recovery environment • Common mental health disorders (e.g., conduct, attention deficit-hyperactivity, depression, anxiety, trauma, self-mutilation and suicidality) • Crime and violence (e.g., inter-personal violence, drug related crime, property crime, violent crime) • HIV risk behaviors (needle use, sexual risk, victimization) • Child maltreatment (physical, sexual, emotional)
NH WA ME MT VT ND MN OR MA ID WI NY SD WY MI RI PA IA CT NE OH NJ NV IN UT IL CA CO WV DE VA KS MO KY MD NC TN OK AZ NM AR SC 0 GA 1 to 10 AL MS 11 to 25 26 to 100 TX LA AK FL HI VI PR One or more state or county wide systems uses the GAIN GAIN Clinical Collaborators Adolescent and Adult Treatment Program DC 7/07
CSAT Adolescent Treatment (AT)Outcome Data Set Recruitment: 1998-2006 (updated annually) Sample: The 2006 CSAT adolescent treatment data set included data with 1 to 4 follow-ups on 12,690 adolescents from 96 local evaluations Levels of Care: Early Intervention, Outpatient, Intensive Outpatient, Short, Moderate & Long term Residential, Corrections Based and Post Residential Outpatient Continuing Care Instrument: Global Appraisal of Individual Needs (GAIN)(see www.chestnut.org/li/gain) Follow-up: Over 80% follow-up 3, 6, 9 & 12 months post intake Funding: CSAT contract 270-2003-00006 and 72 individual grants
Level of Care (n=12,601) Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Type of Treatment (n=12,601) * Data Prior to current AAFT program replicating A-CRA Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Demographics Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Recovery Environment Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Past 90 day HIV Risk Behaviors Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Weekly or More Often Use in the Past 90 Days Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Substance Use Problems Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Prevalence of Past Year Substance Use Disorder by Age Source: Chan, Dennis & Funk in press
Co-Occurring Psychiatric Problems Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Prevalence of Substance, Internalizing and Externalizing Disorders by Age Source: Chan, Dennis & Funk in press
Past Year Violence & Crime *Dealing, manufacturing, prostitution, gambling (does not include simple possession or use) Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Intensity of Juvenile Justice System Involvement Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Relationship of Level of Care to theNumber of Major Clinical Problems Source: CSAT 2006 AT Outcome Data Set (n=12,601); Odds Ratio (OR) of having 5+ of 12 problems (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity)
Relationship of Victimization to theNumber of Major Clinical Problems Source: CSAT 2006 AT Outcome Data Set (n=12,601); Odds Ratio (OR) of having 5+ of 12 problems (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity)
Treatment Outcomes by Level of Care: Days of AOD Abstinence* * Percentages in parentheses are the treatment outcome (intake to 12 month change) and the stability of the outcomes (3months to 12 month change) Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Treatment Outcomes by Level of Care: Recovery* * Recovery defined as no past month use, abuse, or dependence symptoms while living in the community. Percentages in parentheses are the treatment outcome (intake to 12 month change) and the stability of the outcomes (3months to 12 month change) Source: CSAT 2006 AT Outcome Data Set (n=12,601)
Short- Term Resid. \t,s,ts Residential programs start more severe, go down sharply, but then come back over time Long- Term Resid \t,ts Note the sharp “hinge” in outcomes during the active phase of AOD treatment Outpatient \t,s Change in Substance Frequency Scaleby Level of Care\a \a Source: Adolescent Treatment Model (ATM) data; Levels of care coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
Pattern of SA Outcomes is Related to the Pattern of Psychiatric Multi-morbidity Multi-morbid Adolescents start the highest, change the most, and relapse the most 2+ Co-occurring 1 Co-occurring No Co-occurring Number of Past Month Substance Problems 0 12 6 3 Months Post Intake (Residential only) Source: Shane et al 2003, PETSA data
Short- Term Resid. \t,s,ts Long- Term Resid \t,ts Outpatient \t,s Change in Emotional Problem Scale by Level of Care\a Note the lack of a hinge; Effect is generally indirect (via reduced use) not specific \a Source: Adolescent Treatment Model (ATM) data; Levels of care coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
Traumatized groups have higher severity High trauma group does not respond to OP Both groups respond to residential treatment Victimization and Level of Care Interact to Predict Outcomes CHS Outpatient CHS Residential 40 35 30 25 Marijuana Use (Days of 90) 20 15 10 5 0 Intake 6 Months Intake 6 Months OP -High OP - Low/Mod Resid-High Resid - Low/Mod. Source: Funk, et al., 2003
And on average the CYT have moderate effect sizes even with high GVS Green line is CHS OP’s High GVS adolescents; they have some initial gains but substantial relapse Are there other more effective OP programs? 1.00 CYT Total (n=217; d=0.51) 0.80 CHSOP (n=57; d=0.18) 0.60 0.40 0.20 Z-Score on Substance Frequency Scale (SFS) 0.00 -0.20 -0.40 -0.60 -0.80 -1.00 Intake Mon 1-3 Mon 4-6 Mon 7-9 Mon 10-12 Source: CYT and ATM Outpatient Data Set Dennis 2005
Short- Term Resid. \t,s,ts Long- Term Resid \t,ts Outpatient \t,s Change in Illegal Activity Scaleby Level of Care\a Residential Treatments have a specific effect Outpatient Treatments has an indirect effect \a Source: Adolescent Treatment Model (ATM) data; Levels of care coded as Long Term Residential (LTR, n=390), Short Term Residential (STR, n=594), Outpatient/Intensive and Outpatient (OP/IOP, n=560);. T scores are normalized on the ATM outpatient intake mean and standard deviation. Significance (p<.05) marked as \t for time effect, \s for site effect, and \ts for time x site effect.
Randomly Assigns to: Randomly Assigns to: MET/CBT5 MET/CBT5 Motivational Enhancement Therapy/ Motivational Enhancement Therapy/ Cognitive Behavioral Therapy (5 weeks) Cognitive Behavioral Therapy (5 weeks) MET/CBT12 ACRA Motivational Enhancement Therapy/ Adolescent Community Reinforcement Approach(12 weeks) Cognitive Behavioral Therapy (12 weeks) MDFT FSN Family Support Network Multidimensional Family Therapy Plus MET/CBT12 (12 weeks) (12 weeks) Cannabis Youth Treatment (CYT) Experiments Trial 1 Trial 2 Incremental Arm Alternative Arm Source: Dennis et al, 2002
Actual Treatment Received by Condition ACRA and MDFT both rely on individual, family and case management instead of group FSN adds multi family group, family home visits and more case management And MDFT using more family therapy MET/CBT12 adds 7 more sessions of group With ACRA using more individual therapy Source: Dennis et al, 2004
Integrating family therapy was less expensive than adding it Less than average for 6 weeks Less than average for 12 weeks $3,495 $1,776 NTIES Est (6.7 weeks) NTIES Est.(13.1 weeks) Average Episode Cost ($US) of Treatment |--------------------------------------------Economic Cost-------------------------------------------|-------- Director Estimate-----| $4,000 $3,322 $3,500 $3,000 $2,500 Average Cost Per Client-Episode of Care $1,984 $2,000 $1,559 $1,413 $1,500 $1,197 $1,126 $1,000 $500 $- ACRA (12.8 weeks) MET/CBT5 (6.8 weeks) MET/CBT5 (6.5 weeks) MET/CBT12 (13.4 weeks) FSN (14.2 weeks w/family) MDFT(13.2 weeks w/family) Source: French et al., 2002
Adolescent Cannabis Users in CYT were as or More Severe Than Those in TEDS* Source: Tims et al, 2002
Multiple Problems were the NORM Self-Reported in Past Year Source: Dennis et al, 2004
Substance Use Severity was Related to Other Problems 100% 80% 71% 57% 60% 42% 37% 40% 30% 25% 22% 22% 20% 13% 5% 0% Health Problem Acute Mental Acute Attention Conduct Distress* Distress* Traumatic Deficit Disorder* Distress* Hyperactivity Disorder* Past Year Dependence (n=278) Other (n=322) * p<.05 Source: Tims et al 2002
CYT Increased Days Abstinent and Percent in Recovery* 90 90% Days Abstinent 80 80% Percent in Recovery 70 70% 60 60% 50 50% % in Recovery at the End of the Quarter Days Abstinent Per Quarter 40 40% 30 30% 20 20% 10 10% 0 0% Intake 3 6 9 12 *no use, abuse or dependence problems in the past month while in living in the community Source: Dennis et al., 2004
But better than the average for OP in ATM (200 days of abstinence) Similarity of Clinical Outcomes by Conditions Not significantly different by condition. Trial 2 Trial 1 300 50% . 280 40% . 260 30% over 12 months at Month 12 Total days abstinent Percent in Recovery 240 20% 220 10% 200 0% MET/ CBT5 MET/ FSN MET/ CBT5 ACRA MDFT (n=102) CBT12 (n=102) (n=99) (n=100) (n=99) 269 256 260 251 265 257 Total Days Abstinent* 0.28 0.17 0.22 0.23 0.34 0.19 Percent in Recovery** * n.s.d., effect size f=0.06 * n.s.d., effect size f=0.06 ** n.s.d., effect size f=0.12 ** n.s.d., effect size f=0.16 Source: Dennis et al., 2004
Stability of MET/CBT-5 findings mixed at 30 months MET/CBT-5, -12 and ACRA more cost effective at 12 months Integrated family therapy (MDFT) was more cost effective than adding it on top of treatment (FSN) at 30 months Cost Per Person in Recovery at 12 and 30 Months After Intake by CYT Condition Trial 1 (n=299) Trial 2 (n=297) Cost Per Person in Recovery (CPPR) $30,000 ACRA Effect Largely Sustained $25,000 $20,000 $15,000 $10,000 $5,000 $0 MET/ CBT5 MET/ CBT12 FSNM MET/ CBT5 ACRA MDFT $6,437 $10,405 $24,725 $27,109 $8,257 $14,222 CPPR at 30 months** $3,958 $7,377 $15,116 $6,611 $4,460 $11,775 CPPR at 12 months* * P<.0001, Cohen’s f= 1.42 and 1.77 at 12 months ** P<.0001, Cohen’s f= 0.76 and 0.94 at 30 months Source: Dennis et al., 2003; forthcoming
Cumulative Recovery Pattern at 30 months 5% Sustained Recovery 37% Sustained 19% Intermittent, Problems currently in recovery 39% Intermittent, currently not in recovery The Majority of Adolescents Cycle in and out of Recovery Source: Dennis et al, forthcoming
Post Script on CYT • The CYT interventions provide replicable models of brief (1.5 to 3 month) treatments that can be used to help the field maintain quality while expanding capacity. • While a good start, the CYT interventions were still not an adequate dose of treatment for the majority of adolescents – including many who continued to vacillate in and out of recovery after discharge from CYT. • Descriptive, outcome and economic analyses have been published • All five interventions are currently being used in subsequent experiments • The MET/CBT5 intervention has just been replicated in a 38 site study and ACRA is currently being replicated in a 33 site study. • Over 60,000 copies of the CYT manuals have been distributed by NCADI and as many electronic copies have been distributed by CD or the website