Download
1 / 31
530 likes | 2.47k Views
Breech Presentation. By Gabriel Eydt and Jennifer Kasbary.

E N D
Breech Presentation By Gabriel Eydt and Jennifer Kasbary
A 32yoG3T2P0A0L2woman presents for routine prenatal care at 37 weeks. Her pregnancy is complicated by Rh-negative status, depression and a history of LSIL with normal colposcopy in first trimester. Today she reports good fetal movement and denies leaking fluid or contractions. During your examination you measure fundal height at an appropriate 37 cm, and find fetal heart tones located in the upper aspect of the uterus. A bedside ultrasound reveals frank breech presentation. Case
List strategies for management of abnormal fetal presentations,as well as the relative timing of each intervention. Objectives
Types of Breech presentation • Risk Factors for Breech presentation • Management of Breech Agenda
Normally proportionedactivefetus in a normal volume of amniotic fluid will adopt the cephalic presentation near term • This position is the best fit in the intrauterine space. Normal Presentation
Situation where a fetus within the uterus is in any position that is not cephalic • Incidence of breech presentation decreases with increasing gestational age • Common in early pregnancy • Fetus is very mobile • Relatively large volume of amniotic fluid • 20-25% of fetuses under 28 weeks are breech • 7-16% are breech at 32 weeks • 3-4 % are breech at term Malpresentation
(Incomplete) Categories of Breech
At term, 50-70% of breech • Both hips are flexed and both knees are extended (feet are next to the head) Frank Breech
At term, 10-40% of breech • One or both hips are NOT completely flexed • Common in prematurity Footling Breech (incomplete)
At term, 5-10% of breech • Both hips and both knees are flexed Complete Breech
Rare • One or both knees are the presenting part. • Excluded from many classifications Kneeling Breech
Fetal Factors • Fetus too smal relative to environment • Prematurity • Neurologic impairement • Fetal asphyxia • Female • Fetal growth restriction • No room/restricted • Extended fetal legs • Multiple gestation • Short umbilical cord • Fetal abnormalities (anencephaly, dydrocephaly, neck mass) 17% of preterm breech deliveries and 9% in term breech deliveries Risk Factors
Intrauterine/Placental Factors • Uterine anomalies (bicornuate or septateuterus, fibroids) • Space occupying lesion (leiomyomata) • Placental abnormalities (placenta previa) • Multiparity lax abdominal wall and more rounded intrauterine space • Volume of amniotic fluid (polyhydramnios, oligohydramnios) Risk Factors (continued)
Maternal Factors • Maternal anticonvulsant therapy • Older maternal age • Previous breech presentation (9% if the first infant was breech vs 2% if first infant was nonbreech) Risk Factors (continued)
Women often report subcostal discomfort since the fetal head is in the fundus of the uterus. • Diagnosis: Physical examination with the Leopold’s maneuvre… However, this technique is not completely reliable. • If a breech position persist near term or is uncertain… what should we do? How do we know a fœtus is in a breechpresentation?
An ultrasound! This will confirm the presentation and type of breech, estimate the fetal weight, and exclude the presence of a fetal or placental abnormality or an extended fetal head. How do we know a fœtus is in a breechpresentation?
Breech is associated with a higher perinatal mortality and morbidity than cephalic presentation. • The main reasons are: - Increased risk of birth trauma • Increased prevalence of breech presentation among low birthweight/preterm deliveries • Increased prevalence of congenital anomalies and neuromuscular disorders among fetuses in breech presentation Why do we care if a fœtus is in a breech position?
External cephalic version • Spontaneous version can occur before delivery • Educate the mother about the different options and outcomes (vaginal breech delivery vs planned c/s) Antepartum management of Breech
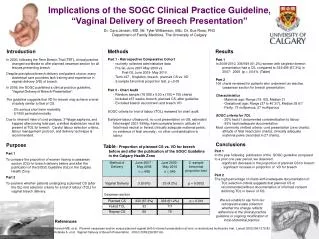
C/S vs vaginal breech delivery … • In North America and Europe c/s deliveries have been on the rise especially since a randomized study called the Term Breech Trial was done in 2000. • It found a «large decrease in perinatal/neonatal mortality and neonatal morbidity, with only a modest increase in short-term maternal morbidity, compared with a policy of planned vaginal delivery». Intrapartum management of breech: C/S
However, both routes of delivery have similar long-term maternal and childhood outcomes and some data suggest some long-term health benefits to being born vaginally. • C/S also has implications for women planning future pregnancies! Intrapartum management of breech: C/S
The Society of Obstetricians and Gynecologists of Canada also allows for selective vaginal breech delivery. Intrapartummanagement of Breech
Vaginal deliveries are mostly spontaneous or slightly assisted. The fetus usually delivers to the umbilicus unassisted, then requires the clinician to perform a rotation of the trunk, apply a suprapubicpressureor a gentle traction on an elbow or knee to help with delivery of the shoulders, limbs, and head. • Women should be in a dorsal or lithotomy position. • Vaginal breech delivery is more likely to be successful if both the mother’s pelvis and the baby are of average proportions. Intrapartum management of breech: vaginal delivery
Ideally the fœtus is in a frank or completebreech • Labour induction may be considered if individual circumstances are favourable. Labour augmentation is not recommended. • Epidural analgesia should not be routinely advised; but it remains the patients choice. • Continouselectronic fetal heart rate monitoring. Intrapartum management of Breech: vaginal delivery
C/S should be considered if there is delay in the descent of the breech at any point in the second stage of labour. Intrapartum management of Breech: vaginal delivery
Intrauterine/Placental Factors • Fetal Factors • Maternal Factors Name one risk factors in each category
Up to Date: G Justus Hofmeyr, MD, Overview of breechpresentation, 2014. http://www.uptodate.com/contents/overview-of-breech-presentation?source=search_result&search=breech+presentation&selectedTitle=1%7E45#H5 G Justus Hofmeyr, MD, Delivery of the fetus in breechpresentation, 2013. http://www.uptodate.com/contents/delivery-of-the-fetus-in-breech-presentation?source=see_link • Medscape • Toronto Notes Schutte MF, van Hemel OJ, van de Berg C, van de Pol A. Perinatal mortality in breech presentations as compared to vertex presentations in singleton pregnancies: an analysis based upon 57819 computer-registered pregnancies in The Netherlands. Eur J Obstet Gynecol Reprod Biol 1985; 19:391. Thorp JM Jr, Jenkins T, Watson W. Utility of Leopold maneuvers in screening for malpresentation. Obstet Gynecol 1991; 78:394. Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet 2000; 356:1375. Resources