Download
1 / 16
210 likes | 766 Views
Case: . HYPERKALEMIA. Group A2. Salient Features. 62 y/o Male Diabetic, Chronic Kidney Disease With proximal weakness Decreased skin turgor. Blood Test. 2. Is this pseudohyperkalemia ? Why or why not?. Pseudohyperkalemia.

E N D
Case: HYPERKALEMIA Group A2
Salient Features • 62 y/o • Male • Diabetic, Chronic Kidney Disease • With proximal weakness • Decreased skin turgor
2. Is this pseudohyperkalemia? Why or why not?
Pseudohyperkalemia • An artificially elevated plasma K+ concentration due to K+ movement out of cells • Factors: • Prolonged use of torniquet (with or withour repeated clenched fist) • Hemolysis • Marked leukocytosis or thrombocytosis
Our patient is not in pseudohyperkalemia • No leukocytosis • No Hemolysis • In Chronic Renal Failure
Rule out: • Pseudohyperkalemia • Trancellular K+ shift • Oliguric Renal failure • Stop NSAIDS and ACEI Assess K+ secretion TTKG <5 TTKG > 10 Inc. distal flow Response to 9α – fludrocortisone • Decreased effective circulating volume • Low – protein diet (decreased urea) TTKG > 10 TTKG < 10 Primary or secondary hypoaldosteronism Hypotension high renin and aldosterone Hypertension Low renin and aldosterone Measure renin & aldosterone levels Pseudohypoaldosteronism K+ sparing diuretics Trimethoprim, pentamide Gordon’s Syndrome (Cl- shunt) Cyclosporine Distal (type 4) RTA
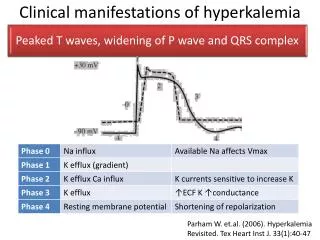
I. Evaluate Hyperkalemia • Confirm the presence of hyperkalemia in patient
II. Determine Urgency Situation • Emergent: if… • Rapid and recent rise in Serum Potassium • Renal insufficiency • Metabolic Acidosis • EKG changes consistent with Hyperkalemia (life – threatening & may be serious) • Treatment: • Individual Medications: • Calcium gluconate • Insulin and Glucose • Kayexalate • Bicarbonate • Dialysis
Calcium gluconate • Stabilize myocardium • Initial dose: 10 ml over 2-5 minutes • Second dose after 5 minutes if no response • Further calcium ineffective unless Hypocalcemia • Insulin and Glucose • Temporarily shift potassium into intracellular space • Insulin Regular 10 units IV • Glucose 50% (D50W) 50 ml (25 grams) • Indicated with insulin if serum glucose <250 mg/dl • Give 1 ampule IV over 5 minutes • consider maintenance (e.g. D5 1/2NS 100 cc/h) • Post initial bolus to cover further insulin
NebulizedAlbuterol • 5 mg/ml • Administer 10-20 mg over 10 minutes • Serum potassium may increase briefly • Bicarbonate • no longer used unless Metabolic Acidosis • Used before as adjunct to Calcium • Consider in severe Metabolic Acidosis • Sodium Bicarbonate 7.5% (44.6 meq) • Give 1 ampule IV over 5 minutes • May repeat every 10-15 min if EKG changes persists • May also add to Glucose infusion • Avoid bicarbonate until Hypocalcemia corrected • Risk of Tetany and Seizures
Non – Emergent: if… • Emergent treatment criteria not met • Serum Potassium <6.0 • Treatment: Enhance postassium excretion • Kayexalate • gastrointestinal excretion: Sodium PolystereneSulfonate (Kayexalate) • Cation-Exchange Resin • Dose: 50 grams • Oral: Administer in 30 ml of Sorbitol • Rectal: Enema activity is faster than oral • Onset: Up to 4-6 hours for oral route • Precautions: • Avoid Sorbitol if bowel necrosis risk • use caution if risk of CHF
Furosemide • Renal excretion • Dose: 20-40 mg IV • Coadminister normal saline if dehydrated • Dialysis • Last option
III. Have a long – term plan • For chronic hyperkalemia patients • Treatment: • Eliminate medication causes of elevated serum potassium • Non-specific therapy • Loop diuretics (Lasix) • Oral Kayexalate chronically • Specific Therapy • Renal Failure (GFR < 10 ml/min) • Restrict dietary Potassium to 40-60 meq/day
Renal Failure and ACE or ARB induced Hyperkalemia • Indications: Metabolic Acidosis • Sodium Bicarbonate • Dose A: 8 meq tabs, 2 tabs twice daily • Dose B: 0.5 to 1 tsp baking soda daily • HyporeninemicHypoaldosteronism • Loop diuretics ( Lasix) • Fludrocortisone 0.1 mg daily • Taper gradually as an outpatient • Restart if Hyperkalemia recurs