Download
1 / 42
420 likes | 534 Views
Antenatal Hospital Encounters and Preterm Delivery, MA 2002-2008. Lizzie Harvey, MPH CDC/CSTE Applied Epidemiology Fellow Massachusetts Department of Public Health June 5, 2012. 1. Background.

E N D
Antenatal Hospital Encounters and Preterm Delivery, MA 2002-2008 Lizzie Harvey, MPH CDC/CSTE Applied Epidemiology Fellow Massachusetts Department of Public Health June 5, 2012 1
Background • MA Infants born <32 weeks gestation made up 1.5% of the birth population but accounted for 63.8% of infant deaths in 2008 • <32 weeks infants have an infant mortality rate (IMR) of 195 deaths/1,000 live births • MA IMR is 5.0 deaths/1,000 live births
Research Priorities • Prematurity is a research priority • IOM Report: “Preterm Birth: Causes, Consequences, and Prevention” • March of Dimes: • Prematurity Research Initiative • “Healthy Babies are worth the wait” campaign • ASTHO Presidential Challenge
Chronic Disease Family History Anemia Stress Family hx of Preterm birth Chronic Hypertension Maternal lbw Maternal Obstetric History Black race Diabetes Low BMI Obesity Short cervix ↑ Maternal age Protective Prior preterm birth Multiple pregnancies Progesterone for prior PTD Pre eclampsia Conceptual Model for Premature Delivery Maternal Behaviors Neighborhood Factors Cervical incompetence Physical Abuse during pregnancy Drug dependency High unemployment Asthma poorly controlled Maternal smoking Stress Lower SES Low maternal Weight gain INCREASED RISK OF PREMATURE DELIVERY Placental Abruption Infections Chorioamnionitis Trichomonasis Bacterial vaginosis
Research Gaps • <32 week population • Low percentage of births • High IMR • Potential for intervention • Course of pregnancy • Hospital encounters
Research Question • In deliveries <32 weeks, are there patterns among antenatal hospital encounters and adverse pregnancy outcomes? • Demographic characteristics • Timing of hospital encounters • Number of hospital encounters • Diagnosis codes of hospital encounters
Methods • Definitions: • Adverse outcome: Any delivery with a fetal death or infant death occurring before 1 year post-delivery • Hospital Encounters: • Emergency Department (ED) • Observational Stay (OS) • Hospital Discharge (HD)
Methods: PELL Data System Vital and Health Status Data Newborn Hearing Screening Birth Defects Registry CORE Program Participation Data Child and Mother deaths Birth Certificate (HD) Birth Mothers Pregnancy-associated deaths WIC Linked birth-infant deaths Early Intervention Cancer Registry Fetal Death (HD) Birth Child PRAMS ART Clinic Data 1998-2008 875,708 births Health Services Utilization Data w/ diagnosis codes & charges Contextual Data Geocoded birth data Non-birth Hospital Discharge Census 2000 Data (and 2010 data) Other Future Datasets: All Payers Data, School, NICU, Medicaid Observational Stays Emergency Department Databases to be added to system
Methods: PELL Data System Vital and Health Status Data CORE Birth Certificate Linked birth-infant deaths Fetal Death 2002-2008 Health Services Utilization Data w/ diagnosis codes & charges Non-birth Hospital Discharge Observational Stays Emergency Department
Methods • Exclusion criteria: • ≥32 weeks gestation delivery • Missing gestational age • HD, OS, or ED admission date outside conception and delivery date • Delivery hospitalization records • Analysis on SAS 9.2: • Frequency distributions • Logistic regressions
567,323 Births, FD, ID 554,603 ≥ 32 weeks 1,494 missing GA 11,226 <32 wks Code by adverse delivery Outcome and delete multiples 9,330 DELIVERIES Results—Data Merging Sorted and merged by child unique identifier Sorted and merged by mother unique delivery identifier
9,330 DELIVERIES 252,853 ED 9,330 DELIVERIES 118,482 OS 9,330 DELIVERIES 32,360 HD Results—Data Merging Deleted non-prenatal hospitalization encounters by GA, delivery date and hospitalization admission date 10,423 DEL+ED 9,788 OS 9,661 HD Merged back to delivery records by unique identifier to capture non-encounters 7,013 NON-ENC. 2,317 DEL. w/ ED 7,788 NON-ENC. 1,542 DEL. w/ OS 7,695 NON ENC. 1,635 DEL. w/ HD 4,013 ED ENC. 2,048 OS ENC. 2,064 HD ENC. Final datasets: 1) 9,330 unique deliveries 2) 11,744 duplicate deliveries with every prenatal hospitalization
Demographics by Delivery Note: % and N do not always equal to 9330 due to missing information in some categories
Initial Results • Exposure: Antenatal hospitalization • 44.0% of deliveries <32 weeks had at least one non-delivery antenatal hospital encounter • Outcome: Adverse pregnancy outcome • 31.2% of deliveries <32 weeks with at least one non-delivery antenatal hospitalizations had an adverse outcome • 34.4% of all deliveries <32 weeks had an adverse outcome
Results: Demographic Characteristics, Hospital Encounters and Adverse Outcomes
Variations by Type of Hospital Encounter p<0.0001 p<0.0001 p=0.20 p<0.0001
Variations by Type of Hospital Encounter p<0.0001 p<0.0001 p<0.0001 p<0.0001
Bivariate Analysis p=0.004 p<0.0001 p<0.0001 p<0.0001
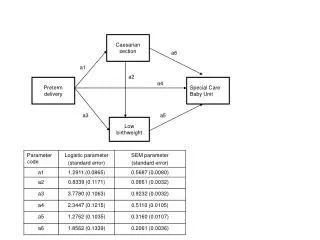
Odds Ratios Adjusted models controlled for: race/ethnicity, education, maternal age, gestational age at delivery, plurality, payer source, method of delivery, prenatal care, nativity
Other Demographic aORs for Adverse Outcomes • Race/Ethnicity: • Black: 0.79 (0.66-0.93) vs. NH white • Gestational age: • <25 weeks: 33.9 (29.1-39.5) vs. 29-31 weeks • 25-28 weeks: 3.61 (3.13-4.15) vs. 29-31 weeks • Plurality: • Twins: 1.61 (1.37-1.90) vs. Singletons • Payer: • Self-care: 1.81 (1.08-3.02) vs. Private • Delivery Method: • Vaginal: 4.34 (3.78-5.00) vs. Primary c-section • VBAC: 4.61 (3.26-6.53) vs. Primary c-section • Nativity: • PR 0.72 (0.59-0.87) vs. US-born • Foreign 1.06 (1.01-1.12) vs. US-born
Number and Duration of Visits: HD Encounters P<0.0001 Mean # visits= 1.26 Mean Length of Stay/visit= 4.07 days
Number and Duration of Visits: OS Encounters P<0.0001 Mean # visits= 1.33 Mean Length of Stay/visit= 0.39 days
Number and Duration of Visits: ED Encounters P=0.0095 Mean # visits= 1.73 Mean Length of Stay/visit= 3.40 hours
No Increased Odds of Adverse Outcomes with Increased ED Encounters
Top 10 Principal Diagnosis Codes with No Adverse Outcomes Threatened premature labor Cervical incompetence Hemorrhage from placenta previa Other conditions, mother, complicating preg/childbirth Mild/NOS pre-eclampsia Premature separation of placenta Premature rupture of membranes Other congenital or acquired abnormality of the cervis Transient hypertension Delayed delivery after spontaneous rupture of membranes HD Diagnosis Codes • Top 10 Principal Diagnosis Codes with Adverse Outcomes • Cervical incompetence • Threatened premature labor • Premature rupture of membranes • Threatened abortion • Hemorrhage from placenta previa • Other conditions, mother, complicating preg/childbirth • Delayed delivery after spontaneous rupture of membranes • Premature separation of placenta • Hyperemesis gravidum with metabolic disturbance • Unspecified hemorrhage in early pregnancy
Top 10 Principal Diagnosis Codes with No Adverse Outcomes Threatened premature labor Other conditions, mother, complicating preg/childbirth Premature rupture of membranes Unspecified antepartum hemorrhage Cervical incompetence Mild/NOS pre-eclampsia Hemorrhage from placenta previa Transient hypertension Other threatened labor Severe pre-eclampsia OS Diagnosis Codes • Top 10 Principal Diagnosis Codes with Adverse Outcomes • Threatened premature labor • Cervical incompetence • Other conditions, mother, complicating preg/childbirth • Premature rupture of membranes • Unspecified hemorrhage in early pregnancy • Threatened abortion • Unspecified antepartum hemorrhage • Twin pregnancy • Intrauterine death • Mild/NOS pre-eclampsia
Top 10 Principal Diagnosis Codes with No Adverse Outcomes Other conditions, mother, complicating preg/childbirth Threatened abortion Unspecified hemorrhage in early pregnancy Mild hyperemesis gravidarum Other specified complications of pregnancy Abdominal pain; unspecified site Infections of genitourinary tract in pregnancy Headache, Facial pain, Pain in head NOS Unspecified antepartum hemorrhage Asthma (bronchial) (allergic NOS) ED Diagnosis Codes • Top 10 Principal Diagnosis Codes with Adverse Outcomes • Other conditions, mother, complicating preg/childbirth • Threatened abortion • Unspecified hemorrhage in early pregnancy • Mild hyperemesis gravidarum • Other specified complications of pregnancy • Infections of genitourinary tract in pregnancy • Unspecified antepartum hemorrhage • Abdominal pain • Headache, Facial pain, Pain in head NOS, • Sprains/strains; neck, Anterior longitudinal (ligament), cervical, Atlanto-axial (joints), Atlanto-occipital (joints), Whiplash injury
Conclusions • 44% of all <32 wk deliveries had ≥1 hospital encounter • Of these deliveries, almost 1/3 will have an adverse outcome • Type of hospital encounter matters: • Deliveries with ≥ 1 ED encounter have a 16% greater risk of adverse outcomes than those with no encounter • OS and HD encounters are protective against adverse outcomes, with 29% and 32% decreased risk, respectively
Conclusions • Demographic: • Gestational age is the driver of poor outcomes • Black mothers and PR born mothers have decreased odds of adverse outcomes • Twins, Self-care payment, and vaginal delivery have increased odds of adverse outcomes • Timing: • Deliveries with adverse outcomes will present sooner in pregnancy with each type of hospital encounter than those without • Women present sooner in the ED than OS or HD • Number: • HD and OS both have decreased odds of adverse outcomes with each additional visit • No increased risk of adverse outcomes with each additional ED visit • Diagnosis: • HD: Cervical incompetence, threatened premature labor, PROM • OS: Cervical incompetence, hemorrhage, threatened abortion • ED: Infections, hemorrhage, sprains/strains
Next Steps • Expand study population • Further refinement of diagnosis coding • Consult with clinicians • Share data by type of hospitalization • Feedback on potential interventions • Exploration of costs associated with hospital utilization
Acknowledgements • Hafsatou Diop, MD, MPH • Xiaohui Cui, PhD • Milton Kotelchuck, PhD, MPH • Maria Vu, MPH • Emily Lu, MPH • Karin Downs, RN, MPH • CDC/CSTE Fellowship
References • CDC Premature Birth: • http://www.cdc.gov/Features/PrematureBirth/ • IOM Report: • National Research Council. Preterm Birth: Causes, Consequences, and Prevention. Washington, DC: The National Academies Press, 2007. • PELL Data System: • https://sph.bu.edu/index.php/Maternal-a-Child-Health/Pregnancy-to-Early-Life-Longitudinal-Linkage-bPELLb/menu-id-452.html • MA Death Statistics: • http://www.mass.gov/eohhs/docs/dph/research-epi/death-report-08.pdf • March of Dimes: • http://www.marchofdimes.com • ASTHO Presidential Challenge: • http://www.astho.org/t/pres_chal.aspx?id=6484
Thank you Contact Information:Lizzie.Harvey@gmail.com