Download
1 / 1
10 likes | 104 Views
Objective Retrospectively test a model-based monitoring method on porcine measurements. Fit subject-specific cardiovascular models from available or inferable ICU data. Track hemodynamic changes due to acute pulmonary embolism (APE) a nd septic shock . (SS).

E N D
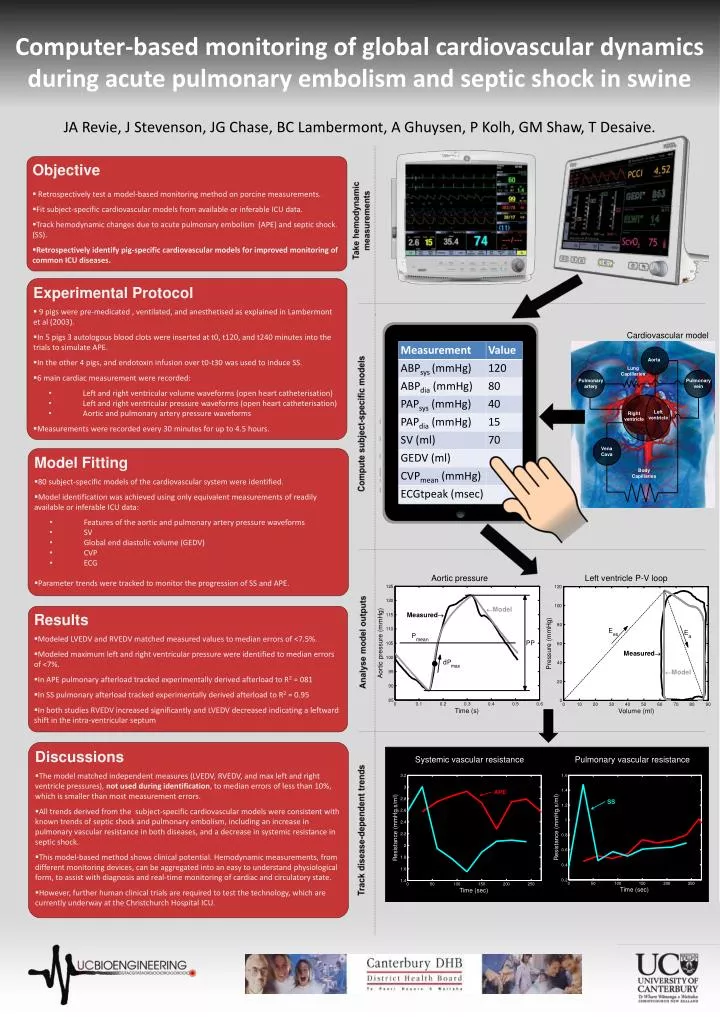
Objective • Retrospectively test a model-based monitoring method on porcine measurements. • Fit subject-specific cardiovascular models from available or inferable ICU data. • Track hemodynamic changes due to acute pulmonary embolism (APE) and septic shock. (SS). • Retrospectively identify pig-specific cardiovascular models for improved monitoring of common ICU diseases. Take hemodynamic measurements • Experimental Protocol • 9 pigs were pre-medicated , ventilated, and anesthetised as explained in Lambermont et al (2003). • In 5 pigs 3 autologous blood clots were inserted at t0, t120, and t240 minutes into the trials to simulate APE. • In the other 4 pigs, and endotoxin infusion over t0-t30 was used to induce SS. • 6 main cardiac measurement were recorded: • Left and right ventricular volume waveforms (open heart catheterisation) • Left and right ventricular pressure waveforms (open heart catheterisation) • Aortic and pulmonary artery pressure waveforms • Measurements were recorded every 30 minutes for up to 4.5 hours. • . Computer-based monitoring of global cardiovascular dynamics during acute pulmonary embolism and septic shock in swine Cardiovascular model Aorta Lung Capillaries Pulmonaryartery Pulmonaryvein Compute subject-specific models Left ventricle Right ventricle • Model Fitting • 80 subject-specific models of the cardiovascular system were identified. • Model identification was achieved using only equivalent measurements of readily available or inferable ICU data: • Features of the aortic and pulmonary artery pressure waveforms • SV • Global end diastolic volume (GEDV) • CVP • ECG • Parameter trends were tracked to monitor the progression of SS and APE. Vena Cava BodyCapillaries Aortic pressure Left ventricle P-V loop JA Revie, J Stevenson, JG Chase, BC Lambermont, A Ghuysen, P Kolh, GM Shaw, T Desaive. • Results • Modeled LVEDV and RVEDV matched measured values to median errors of <7.5%. • Modeled maximum left and right ventricular pressure were identified to median errors of <7%. • In APE pulmonary afterload tracked experimentally derived afterload to R2= 081 • In SS pulmonary afterload tracked experimentally derived afterload to R2= 0.95 • In both studies RVEDV increased significantly and LVEDV decreased indicating a leftward shift in the intra-ventricular septum Analyse model outputs • Discussions • The model matched independent measures (LVEDV, RVEDV, and max left and right ventricle pressures), not used during identification, to median errors of less than 10%, which is smaller than most measurement errors. • All trendsderived from the subject-specific cardiovascular models were consistent with known trends of septic shock and pulmonary embolism, including an increase in pulmonary vascular resistance in both diseases, and a decrease in systemic resistance in septic shock. • This model-based method shows clinical potential. Hemodynamic measurements, from different monitoring devices, can be aggregated into an easy to understand physiological form, to assist with diagnosis and real-time monitoring of cardiac and circulatory state. • However, further human clinical trials are required to test the technology, which are currently underway at the Christchurch Hospital ICU. Systemic vascular resistance Pulmonary vascular resistance APE SS Track disease-dependent trends