Download
1 / 51
610 likes | 1.15k Views
Emergency Management of Acute Decompensated Heart Failure. Hani Ramadan PharmD Candidate 4/19/2007 Beaumont Hospital Royal Oak, MI. CC: Weakness and Shortness of Breath . 4/06/07 (ER) HPI:

E N D
Emergency Management of Acute Decompensated Heart Failure Hani Ramadan PharmD Candidate 4/19/2007 Beaumont Hospital Royal Oak, MI
CC:Weakness and Shortness of Breath. 4/06/07 (ER) HPI: BH is a 95 year-old female with a known history of CHF, HTN, anxiety. Patient presents with altered mentation along with swelling in the legs and arms. PMH: HTN, CVA, chronic atrial fibrillation, anxiety.
Allergies:PCN (rash) SH:Lives at home, has a 24 hour caregiver. Medications at Home:Atenolol 25 mg qd, pantoprazole 40mg qd, ASA 81 mg qd, lorazepam 1 mg qhs, clopidogrel 75 mg qd, acetaminophen 500 mg qid prn, ciprofloxacin 500mg bid. Physical assessment: 3+ edema from waist down. VS:H=4’11” W=50.0kg T= 36oC, P= 96, RR=18,BP=114/86 HEENT:conjunctivae and lids have no pallor and no jaundice. Pupils equal, round and reactive to light and accomodation. Ears, nose and throat normal.
Lungs:bilateral basilar crackles. CV:heart rhythm irregular. Abd:soft.no n/v/d, no hepatosplenomegaly. Neuro:lethargic. GCS:14. Labs: Na 139 WBC 10.5 Scr 1.8 BNP 1343 K 4.1 HGB 9.6 BUN 30 AG 9 Cl 108 HCT 48 Plt 296 CK 171 MB 6.4 X-Ray: small left effusion, atelectasis, no pneumothorax. EKG:atrial fibrillation w ventricular response, with T wave inversions.
Physician’s assessment/plan: • Congestive Heart Failure: Patient will receive IV diuretics and monitor for electrolytes. 2. UTI: Continue Cipro until the completion of the course. • Abnormal cardiac enzymes: Represent myocardial injury. Cardiology consulted. • Acute Renal insufficiency: Monitor creatinine, diuresis and BP.
Epidemiology Mortality is approx. 50% at 5 years ~ 5 million Dx in US ~550 000 new cases/yr ~ 1 million hospitalizations/ yr Economic Costs approx. 29.6 billion $ (direct and indirect costs) Heart disease and stroke statistics- 2006 Update, American Heart Association
Objectives • Review the pathophysiology of ADHF. • Describe the clinical presentation of ADHF. • Apply effective therapeutic strategies using consensus guidelines from the (HFSA) and the (ESC). • Examine the clinical evidence of milrinone and niseritide in the treatment of ADHF. • Evaluate the appropriateness of treatment.
ADHF • Rapid onset of signs and symptoms secondary to abnormal cardiac function due to systolic, diastolic dysfunction, abnormalities in cardiac rhythm or to pre-load and after-load mismatch. • De novo or acute decompensation of CHF. • ~50% of patients have a systolic blood pressure >140mmHg. • ~46% of patients have a preserved (LVEF). • Patients often present with multiple co-morbidities. • Killip Classification. • Forrester Classification. • Clinical Severity Classification.
Pathophysiology • LV dysfunction: • Accumulation of fluid. • Decrease in CO Hypoperfusion. • Reciprocal Activation of (RAAS) • Na, water retention. • AGII ET1 + Vasopressin. • Reflex activation of SNS: Epi, NE.
Killip Classification • Stage I: No clinical signs of decompensation. • Stage II: Heart failure. Rales, S3, PVH. • Stage III: Severe heart failure. Pulmonary edema with rales throughout the lung fields. • Stage IV: Cardiogenic Shock: Hypotension, peripheral vasoconstriction, oliguria, cyanosis and diaphoresis.
Forrester Classification Cardiac Index (L/min/m2) 18 mmHg 5 4 3 2.2L/min/m2 2 1 10 20 30 Pulmonary Capillary Wedge Pressure (mmHg) Nohria A et al. JAMA.2002:287; 628-40
Common Precipitating Factors • Pulmonary embolus • COPD • Anemia • Thyroid disorders • Nondihydropyridine CCB • Sodium retaining medications • Medication non-adherence. • Dietary indiscretion. • Infection (pneumonia, UTI, etc.) • Renal failure. • Cardiotoxic/nephrotoxic medication. • Uncontrolled hypertension • Cardiac Arrhythmias • Myocardial ishemia • Valvular disease
Differential Diagnosis • Pneumonia • Reactive airway disease • Pulmonary embolus
Diagnosis • Diagnosis of ADHF should be primarily based on signs and symptoms.(C)
Diagnosis Low-Intermediate clinical suspicion of ADHF BNP (A) BNP > 500pg/ml BNP 100-500pg/ml BNP < 50-100pg/ml ADHF more likely Likely, but consider other causes ADHF less likely
Predictors of Mortality • BUN > 43 mg/dl • SBP < 115 mmHg • sCr >2.75 mg/dl } Highest risk of mortality Fonarow GC et al. JAMA. 2005;293:572-80
Goals of Therapy • Improve symptoms and signs of congestion and/or hypoperfusion. • Reverse hemodynamic abnormalities. • Identify the etiology. • Minimize side effects. • Optimize therapy. • Length of stay, mortality, time to hospital readmission.* • Educate patients on medications and self assessment of HF.
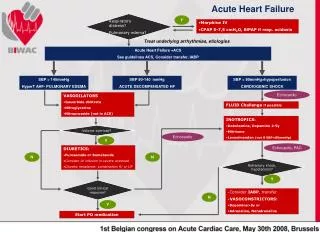
Treatment Strategy • Establish a Diagnosis • Oxygen and Ventilatory Assistance • Symptom Relief • Anticoagulation • Hemodynamic Support: • Diuresis/Fluids • Vasodilators • Inotropes • Vasopressors • Assess Patient Response • Anti-infectives • Glucose Control
The Principle Reduce Fluid Overload Reduced Preload: (E-DVf), PCWP • Diuretics • Inotropes • Vasodilators Increase Contractility Increase CO, EF, Perfusion Reduce Preload Reduce Afterload
Assess Signs/Symptoms/Determine Hemodynamic Status EC Interventions: Cardiac panel: (CBC w/diff & platelets, SMA-7 CK-MB, Glucose), TSH, Pox, ECG, BNP, X-ray Abnormal Normal Consider alternative diagnosis Evaluate cardiac function by2DE Does Patient presents with Distress or pain? Characterize type and severity yes Is patient hypoxic? Morphine 3 mg IVPBIIbB Yes Does patient present with ischemic chest pain resistant to opiates or tachycardia? No but difficult breathing OxygenC CPAP NIPPV Metoprolol 5 mg IV* IIbC
Volume Overloaded (A) Moderate Volume Overload IV Diuretics Furosmide 20-40 mg Bumetanide 0.5-1.0 mg Torasemide 10-20 mg IB/B Consider Dopamine <2-3 ug/kg/min IIbC Ultrafiltration or Hemodialysis C Inadequate Response < 250-500 ml within 2 hours Consider Severe Volume Overload(B) Or Low Cardiac Output(C) Na/fluid restriction Add HCTZ 25-50 mg bid, or Metolazone 2.5-10 mg qd, or Spironolactone 25-50 mg qd IIbC/C Refractory to loop + thiazides
(B) Severe Volume Overload SBP>90 mmHg IV Diuretics +/- IV Vasodilators Furosmide 40-100 mg IV then 5-40 mg/h inf. Bumetanide 1-4 mg Torasemide 20-100 mg PLUS Nitroglycerin 5-10 ug/min inf.* Class IIbC/C
(C)Low Cardiac Output SBP >100 mmHg SBP 85-100 mmHg SBP < 85 mmHg Volume repletion Inotrope IIaC/C And/or Dopamine >5ug/kg/min Vasodilator (NTG, Nitroprusside)C On a B-blocker chronically? Yes/No No or D/C Consider D/C or reducing dose if sign of excessive dose are suspected Dobutamine IIaCC 2-3 ug/kg/min inf. -20ug/kg/min inf. Hypoperfusion resolving? Milrinone 25-75ug/kgIVPB over10-20min Then 0.37-0.75ug/kg/min inf. IIbC/IIaC*C yes No (D) Tapper off dobutamine by steps of 2 ug/kg/min qod +optimize tx with hydralazine and/or ACE-I
(D)Unresolved hypoperfusion Transient use of Vasopressor therapy Use of invasive hemodynamic monitoring C Epinephrine 0.05-0.5 ug/kg/min inf. Norepinephrine 0.2-1ug/kg/min +/- dobutamine 0.05-0.5 ug/kg/min inf.
Monitoring Parameters • Oxygen Saturation • CBC • BP • ECG • BNP • Signs: • Edema, Rales, Ascites, Hepatomegaly, JVD • Symptoms: • Orthopnea, PND, Dyspnea, Fatigue, Cough • Negative/positive balance • Electrolytes • Urinalysis • BUN/Scr • ABG
(OPTIME-CHF) Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure JAMA, March 27 2002: 287(12);1541-1547 Objective:To prospectively test whether a strategy that includes short–term use of milrinone in addition to standard therapy can improve clinical outcomes of patients hospitalized with an exacerbation of chronic heart failure.
Study Design • Prospective randomized double-blind placebo-controlled trial. • ITTA. • Similar baseline characteristics. • Randomization to a 48 hour infusion of either milrinone (n = 477) or placebo ( 472). • Milrinone treatment arm: Started with an initial infusion of 0.5ug/kg/min for 48hrs. (Rate adjusted to 0.375 ug/kg/min)
Outcome Measures • Primary Efficacy Outcome: • The total number of days hospitalized for cardiovascular causes or days decreased within the 60 days after randomization. • Secondary endpoints: • Failed therapy because of adverse events. • Failed therapy because of worsening heart failure. • Proportion of patients achieving target doses of ACE-I therapy. • Time to achieve target ACE-I dose. • Symptom improvement in HF score.
Results • Treatment with milrinone did not reduce the primary endpoint of days hospitalized for cardiovascular causes within 60 days compared with placebo.
Results (cont’) Treatment failure cause at 48 hours: Adverse event Events during hospitalization: MI New atrial fibrillation/flutter Ventricular tachycardia/fibrillation Sustained hypotension Placebo (n=472) Milrinone (n = 477) P value 2.1% 12.6% <0.001 0.4% 1.5% <0.18 1.5% 4.6% <0.04 1.5% 3.4% <0.06 3.2% 10.7% <0.001
Limitations • Study did not directly address patients with acutely decompensated chronic heart failure for whom inotropic therapy is essential. • Non-formal therapeutic protocol.* • Confounding variables.
Conclusions • Results do not support the routine use of milrinone in patients hospitalized with an exacerbation of chronic heart failure.
(VMAC)Intravenous Nesiritide vs Nitroglycerin for Treatment of Decompensated Congestive Heart Failure Objective: To compare the efficacy and safety of intravenous nesiritide, intravenous nitroglycerin and placebo.
Study Design • Randomized double-blind, double dummy trial. • Patients were stratified to catheterized (n=246) and non-catheterized (n= 243) • Patients were then randomized to fixed dose nesiritide, adjustable dose niseritide, nitroglycerin or placbo for the first 3 hours. • After 3 hours patients were in the double dummy design of nesiritide and nitroglycerin treatment arms.
Outcome Measures • Primary Endpoint: Change in PCWP and patient’s self-evaluation of dyspnea from baseline at 3hours. • Secondary Endpoints: • Onset of effect on PCWP • Effect on PCWP 24 hrs after the start of study drug • Self-assessed dyspnea and global clinical status • Overall safety profile.
Results • Reduction in PCWP was greater in the nesiritide group with the first measurement. • Beyond 24hr the difference in PCWP between nesiritide and nitroglycerin was insignificant. • Improvement in dyspnea and global clinical status scores in the nesiritide and nitroglycerin were not significantly different at any time. • HA was more common in the Nitroglycerin group.
Limitations • Heterogenous patient population* • Therapeutic protocol. • Assessment of mortality/morbidity
Conclusion • When added to standard care in hospitalized patients with ADHF, nesiritied improves hemodynamic function and some self-reported symptoms more effectively than intravenous nitroglycerin.
CC:Weakness and Shortness of Breath. 4/06/07 (ER) HPI: BH is a 95 year-old female with a known history of CHF, HTN, anxiety. Patient presents with altered mentation along with swelling in the legs and arms. PMH: HTN, CVA, chronic atrial fibrillation, anxiety.
Allergies:PCN (rash) SH:Lives at home, has a 24 hour caregiver. Medications at Home:Atenolol 25 mg qd, pantoprazole 40mg qd, ASA 81 mg qd, lorazepam 1 mg qhs, clopidogrel 75 mg qd, acetaminophen 500 mg qid prn, ciprofloxacin 500mg bid. Physical assessment: 3+ edema from waist down. VS:H=4’11” W=50.0kg T= 36oC, P= 96, RR=18,BP=114/86 HEENT:conjunctivae and lids have no pallor and no jaundice. Pupils equal, round and reactive to light and accomodation. Ears, nose and throat normal.
Lungs:bilateral basilar crackles. CV:heart rhythm irregular. Abd:soft.no n/v/d, no hepatosplenomegaly. Neuro:lethargic. GCS:14. Labs: Na 139 WBC 10.5 Scr 1.8 BNP 1343 K 4.1 HGB 9.6 BUN 30 AG 9 Cl 108 HCT 48 Plt 296 CK 171 MB 6.4 X-Ray: small left effusion, atelectasis, no pneumothorax. EKG:atrial fibrillation w ventricular response, with T wave inversions.
Physician’s assessment/plan: • Congestive Heart Failure: Patient will receive IV diuretics and monitor for electrolytes. 2. UTI: Continue Cipro until the completion of the course. • Abnormal cardiac enzymes: Represent myocardial injury. Cardiology consulted. • Acute Renal insufficiency: Monitor creatinine, diuresis and BP.
References • Adams KF et al. J Card Fail. 2006; 12:10-38. • Nieminem MS et al. Eur Heart J 2005; 26:384-416. • Cherney D. et al. Management of Patients with Hypertensive Urgencies and Emergencies. JGIM 2002;17:937-944. • Krum H. et al. New and Emerging Drug Therapies for the Management of Acute Heart Failure. Internal Medicine Journal 2003;33:515-520. • Peacock W. F. et al. Acute Emergency Department Management of Heart Failure. Heart Failure Reviews 2003;8:335-338. • Wang T. J. et al. Plasma Natriuretic Peptide Levels and the Risk of Cardiovascular Events and Death. NEJM 2004;350(7):655-663. • Alan S. M. et al. Cardiac Natriuretic Peptides: A Proteomic Window to Cardiac Function and Clinical Management. Reviews In Cardiovascular Medicine 2003;4(4):S3-S12. • Millane T. et al. ABC of Heart Failure: Acute and Chronic Management Strategies. BMJ 2000;320:559-562. • DiDomenico RJ.The Annals of Pharmacotherapy 2004 April:38;649-660 • Gregg C. F. et al. The Treatment Targets in Acute Decompensated Heart Failure. Reviews In Cardiovascular Medicine 2001;2(2):S7-S12. • Diagnosis and Treatment of Acute Heart Failure. Retrieved from www.guidelines.gov 2002. • Acute Exacerbation of CHF. Australian Heart Foundation 2006:43-49. • Rapid Optimization: Strategies for Optimal Care of Decompensated Congestive Heart-Failure Patients in the Emergency Department. Reviews In Cardiovascular Medicine 2002;3(4):S41-S48. • Hunt S. A. et al. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1995 Guidelines for the Evaluation and Management of Heart Failure). ACC/AHA Practice Guidelines 2001:1-55. • VMAC Investigators. JAMA. 2002;287:1531-40.
Level of Evidence • Heart Failure Society of America: • Level A: Randomized controlled clinical trials • Level B: Cohort and case-control studies • Level C: Expert opinion • European Society of Cardiology: Class I Evidence and/or general agreement that a given diagnostic procedure/treatment is beneficial, useful and effective; • Class II Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the treatment; • Class IIa Weight evidence/opinion is in favour of usefulness/efficacy; • Class IIb Usefulness/efficacy is less well established by evidence/opinion; • Class III Evidence or general agreement that the treatment is not useful/effective and in some cases may be harmful. • Levels of Evidence • Level of Evidence A Data derived from multiple randomized clinical trials or meta-analysis • Level of Evidence B Data derived from a single randomized clinical trial or large non-randomized studies Level of Evidence C Consensus of opinion of the experts and/or small studies; retrospective studies and registries