Download
1 / 26
320 likes | 519 Views
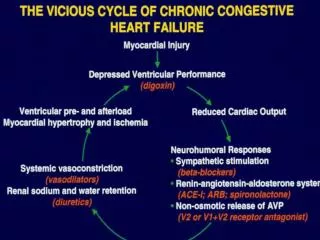
Telemonitoring for Heart Failure Evidence & Practice. Professor John G.F. Cleland Department of Cardiology, Hull Y o rk Medical School University of Hull Kingston-upon-Hull UK. Conflict of Interest: I have received honoraria and/or research support from Philips, Bosch, GE, Alere and St Jude.

E N D
Telemonitoring for Heart FailureEvidence & Practice Professor John G.F. Cleland Department of Cardiology, Hull York Medical SchoolUniversity of Hull Kingston-upon-Hull UK Conflict of Interest: I have received honoraria and/or research support from Philips, Bosch, GE, Alere and St Jude
Audit Survival of Patients with a Primary Discharge Diagnosis of Heart Failure England & Wales 2009-2010 About 1 million people affected in the UK ~450,000 admissions per year (65,000 in first diagnostic position) N = 19,240 (about 30% of all expected cases) Median age 79 years <65 years ~3,000 65-75 years ~4,000 75-85 years ~7,000 >85 years ~5,000 Cleland et al HEART 2011
TeleHealthWhy is it Likely to Become Essential? • More patients with long-term conditions • More older people • Longer survival with illness • Better primary & secondary prevention • Fewer professionals to provide health-care • Smaller proportion of population of working age • Loss of migrant workforce as economies rival UK • Better paid or more attractive / less stressful jobs • More monitoring required • Higher expected standards of care • More treatments that need to be monitored • More things that can be monitored
TeleHealthWhy is it Likely to Become Essential? • Patient preference & Convenience • Patients, Carers, Staff • Reduced Costs • Buildings, Staff, Transport • Environmental impact • Transport • Parking • Buildings • Better record keeping !!!!!!!!!!!!!!!!!!!!!!!
The Opportunity of Chronic Illness • Most patients soon learn routines • Or have relatives / friends that do • Most patients are interested in maintaining or improving their health • Patients are an ‘inexpensive’ but neglected health-care provider opportunity • Invest in patients • Education • Active Partnership • Empowerment
TeleHealth - What Might it Achieve? Ultimate Intermediate
TEN-HMSThe Trans-European Network–Home-Care Management SystemPatients about to be discharged from hospital after an exacerbation of chronic heart failure 54% of Patients Aged >70 years (Published JACC 2005)
TEN-HMS Reduction in Mortality NTS or HTM v UC Absolute 16.4% Relative 36 % Mortality No reduction in hospitalisation Shortening of hospital stay with HTM p < 0,05 Cleland et al JACC 2005
TEN-HMS “ How do you feel about your health since receiving Telemonitoring? “ much safer no change much more anxious more anxious Undef. safer
TEN-HMS Achieving Therapeutic Target Patient Clinical Status *** *** *** % 240 Days 120 Days 240 Days *** differences between HTM and other groups. No difference between UC and NTS
TEN-HMS: Total Patient Contacts Contacts Per 1,000 Days Alive and Out of Hospital # P<0.01 HTM v NTS # under-reporting of events likely in this group
Structured Telephone Supportn = 5,563(Cochrane Review) All-Cause Hospitalisation HR 0.77 (0.68-0.87.01); p<0.0001 Mortality • New Trials • Tele-HF • TEHAF HR 0.88 (0.76-1.01); p=0.08 Inglis et al 2010
Home Telemonitoringn = 2,710(Cochrane Review) All-Cause Hospitalisation HR 0.91 (0.84-0.99); p=0.02 • New Trials • TIM-HF • COMPASS • CHAMPION • SENSE-HF Mortality HR 0.66 (0.54-0.87); p<0.0001 Inglis et al 2010
Major Problems with RCTs of Service Delivery • Technology differs • Telephone Support including Voice Activated Systems • Physiological telemonitoring • Implanted or Not • Care usually improves if it is the focus of attention • Effect in control group • Beware: “before v after” comparisons • Lack of integration into existing services • Puts innovative interventions at a disadvantage • Selection of patients at low risk with modern treatment
Percent of Days Lost To Hospitalisation or Death TEHAF (12 months) TIM-HF (26 months) TEN-HMS (15 months) 8.9% 8.4% 37.0% 21.3% 22.6% 4.5% 6.1%
What Have We Done for TeleHealth in Hull? • Established • International reference site (LifeLab) for HF epidemiology & research • International reputation for research excellence in telehealth • A model telehealth service • Grants • TEN-HMS • Four FP7 grants relating to telehealth & heart failure • EDRF • Industry Partnerships • Philips, GE, Bosch, Cardiomems, St Jude + others • Publications • >500 PubMed citations in related fields • TEN-HMS, Concept Papers, Editorials • Systematic Reviews (EJHF, BMJ & Cochrane) • Inventions • Dynamic risk analysis • Complex management algorithms
MEMS-based pressure sensor The Hull Model for TeleHealth • HeartCycle • Heart Failure • Post-MI Rehab Device Implant Non-Invasive Home Monitoring Community TeleKiosks Screening Long-Term Conditions
Services for Patients with Heart FailureThe Kingston-upon-Hull Model Heart Failure Discharge Nurse Heart Failure Telemonitoring Nurse Voluntary Patient-Support Organisations Community Heart Failure Specialist Nurses Patients in Hospital Patients at Home Family Doctor (NT-proBNP) Specialist Clinics
Cost-Effectiveness of TeleHealth (Hull)
Where Next? • Interactive TV • New monitoring technologies • Implanted devices • More intelligent use of the patient data • Investing in patients as health-care providers Centre for Telehealth
The Hull Heart Failure Life-Lab30,000 patient-years of follow-upLargest, Longest Follow-up, Epidemiologically-Representative Cohort of Heart Failure in the WorldRich in phenotyping, serial biomarker and outcome data
Shift from crisis detection to health maintenance Health Maintenance Envelope More ‘optimistic’ Better way to engage/motivate patients More active management More activity likely to hold ‘actors’ attention Clinical calibration Addresses the issue of false alerts Personalised Careplan Treatments Ideal monitoring envelope HeartCycle Programme
Motivation: feedback on measures and trends, what they mean and what to do about them Education: on healthy lifestyle, reasons for treatments, self management Health-Care Provider Secondary Loop Patient / Carer Analysis Primary Loop 70% of Care Decisions ‘Monitor’ Intelligent, integrated, multi-measure (time & type) personalised analysis Communication System
Opportunities for TeleHealth • Change in Philosophy • Investment in patients (rather than experts) • Patients as first and possibly main tier of healthcare • Communication • Patient, community health & social services, specialists • Common health record • Checked (at least in part) by the patient themselves • Decision support analysis • Patient & professional support • Research potential +++ • Healthcare innovation • Pharmaceutical industry especially • Route to faster (ethical) adoption • Convenience & Preference • Patient, Carer, Health Professional • Environmental impact
Conclusion The first era of telemonitoring is over Time to move from Crisis Detection to Health Maintenance