Download
1 / 26
260 likes | 541 Views
AN OVERVIEW OF SPEECH AND LANGUAGE DEVELOPMENT Nicola Hall Speech and Language Therapist. Agenda. Background to speech and language therapy What is communication? Where the breakdown can occur Speech and Language Therapy Input Questions and Answers. Background

E N D
AN OVERVIEW OF SPEECH AND LANGUAGE DEVELOPMENT Nicola Hall Speech and Language Therapist
Agenda • Background to speech and language therapy • What is communication? • Where the breakdown can occur • Speech and Language Therapy Input • Questions and Answers
Background What does a Speech and Language Therapist do? • A Speech and Language Therapist is a person trained to work with people of any age with communication or swallowing difficulties. • We are trained to deal with neonates up to elderly • This may include: • Assessment • Diagnosis • Treatment • Pre-referral Work and Health Education
What is Communication? What do speech and language therapists consider?
Attention STAGE 1 – 1ST yr: Period of extreme distractibility STAGE 2 – 2nd yr: The child can concentrate for some time on a concrete task of his own choosing STAGE 3 – 3rd yr: Attention is single channelled, but more flexible STAGE 4 – 4th yr: Child can control his own attention focus STAGE 5 – 5th yr: The child’s attention becomes two channelled STAGE 6 – 6th yr: Integrated attention is well established and well sustained
Language • STAGE 1: DISCOVERER (birth to 8 months) The infant goes from communicating reflexively to becoming really interested in others and wanting attention. She does not yet know how to send messages directly to another person to get what she wants. • STAGE 2: COMMUNICATOR (8 to 13 months) The infant sends purposeful messages directly to others using a combination of eye gaze, facial expressions, sounds and gestures. She becomes very sociable. • STAGE 3: FIRST WORDS USER (12 to 18 months) The infant cracks the language code and begins to use single words.
STAGE 4: COMBINER (18 to 24 months) The child demonstrates a burst in vocabulary and begins to combine words. She also starts to take more turns in conversation • STAGE 5: EARLY SENTENCE USER (2 to 3 years) The child progresses from using two-word combinations to five-word sentences and can now hold short conversations • STAGE 6: LATER SENTENCE USER (3 to 5 years) The child uses long, complex sentences and holds conversations
Speech Development Where there are 2 sounds at the beginning of a word, eg st, sn, br, fl, these take longer to develop. Often not before 5yrs old
Fluency • Children will often stop, pause, start again and stumble over words when they are learning to talk. • Between the ages of two and five years it is normal for a child to repeat words and phrases and hesitate with ‘um’s and ‘er’s when they are thinking what to say next. • About 5 in every 100 children stammer for a time when they are learning to talk. Many find it easier to talk as they get older. Others continue to find talking difficult and often get stuck. • More boys than girls have persistent stammers.
Warning bells: • does anyone else in the family have (or had) a stammer? • has the child been stammering for longer than 6 months? • is the child beginning to do other actions eg screwing their face up, blinking, foot tapping, word avoidance to ‘help’ their speaking? • has the child had difficulties with speech and language skills previously?
Social Skills • Can be the result of underlying language difficulty • ASD • Aspergers Syndrome • Social Communication • Social Interaction • Play skills
Eating and Drinking - Risk Factors • Prematurity or low birth weight • Syndromes – Down Syndrome, Prader Wili • Neurological Disorders – cerebral palsy, meningitis • Acquired trauma – head injury • Delayed introduction of textured food • Structural problems – cleft lip/palate, tracheostomy • Heart disease • Gastro-intestinal conditions
Poor feeding Difficulties chewing Difficulties in drinking Refusing food/drink Coughing/choking Eyes watering Colour change Gurgly/wet voice Breathing difficulties Gagging/vomiting Frequent chest infections Poor weight gain General distress around eating/drinking Avoiding certain foodstuffs eg. Crunchy things, lumps that require lots of chewing Prolonged feeding times Signs and Symptoms
Who Should I Refer? Not just the disorder but how this impacts on the individual child and family • How does this affect the child’s development in everyday life? • What does this stop the child/family doing? • How does this make the child/family feel?
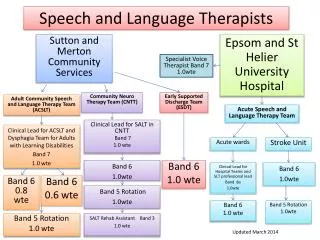
Role of the Speech & Language Therapist • Pre-referral (Public Health) • Referral • Open referral system • Triage • Assessment • Determine level of SLT risk • Diagnosis & description • Intervention plan • Intervention • Direct • Indirect • Discharge
General Advice • Suggest nursery placement for children not yet in education. • In Greater Glasgow give Helpline number to parents • In all situations, asking children to repeat what they are saying is likely to increase stress. Advise parents not to pressure the child into repeating or speaking to people. Listen to WHAT the child is communicating not HOW • Consider referring to audiology if any concerns about hearing. • Consider involving other services eg CDC if any concerns regarding social interaction.
Consultation & Advice Line Wednesday: 1.00pm to 4.00pm274 2075 Anyone involved with a child can call (Glasgow only at the moment) Staffed by an experienced speech and language therapist who can give general advice and/or advise on appropriateness of referral Friday: 9.30am to 11.30am 531 6843
BilingualFamilies Where there are 2 (or more) languages being spoken….. • Never advise giving up mother tongue • The adults should be consistent with the languages, try not to mix them • SLT would be involved if child has problems in all languages, not just learning English
Useful Websites www.talkingpoint.org www.rcslt.org www.hpc-uk.org www.stammering.co.uk www.talktoyourbaby.org.uk www.afasic.org.uk www.nas.org.uk
QUESTIONS & ANSWERS nicolahall@nhs.net