Download
1 / 1
10 likes | 123 Views
No. 007. The PRIAS Study In Australia One Institution ’ s Experience. Jeremy P Grummet, Matthew J Lin The Alfred Hospital. Introduction

E N D
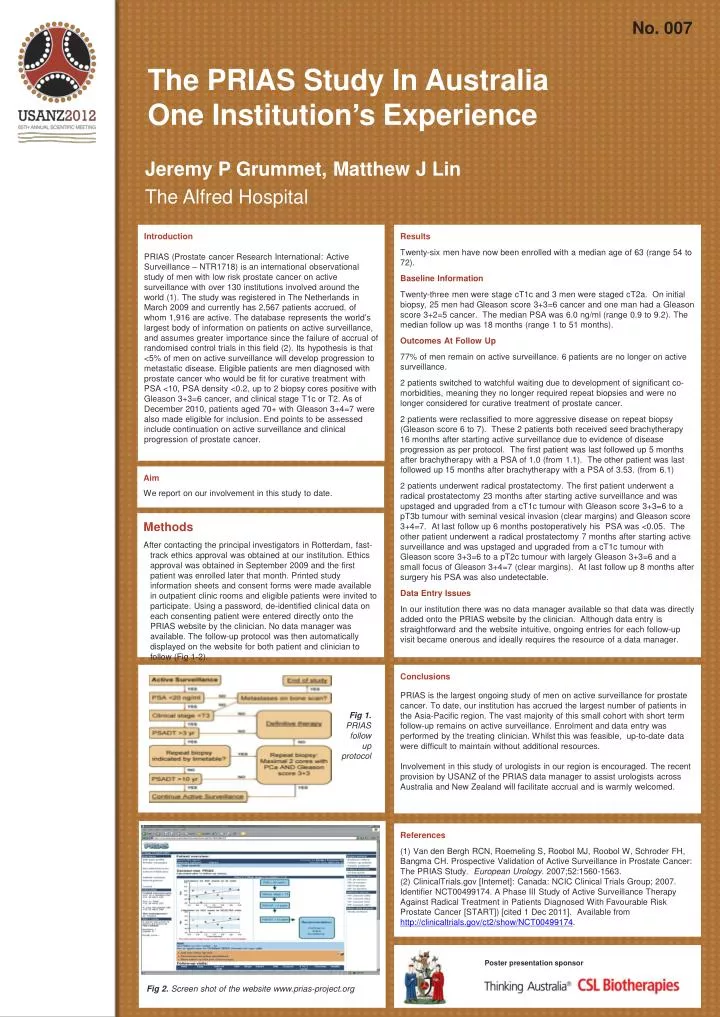
No. 007 The PRIAS Study In Australia One Institution’s Experience Jeremy P Grummet, Matthew J Lin The Alfred Hospital Introduction PRIAS (Prostate cancer Research International: Active Surveillance – NTR1718) is an international observational study of men with low risk prostate cancer on active surveillance with over 130 institutions involved around the world (1). The study was registered in The Netherlands in March 2009 and currently has 2,567 patients accrued, of whom 1,916 are active. The database represents the world’s largest body of information on patients on active surveillance, and assumes greater importance since the failure of accrual of randomised control trials in this field (2). Its hypothesis is that <5% of men on active surveillance will develop progression to metastatic disease. Eligible patients are men diagnosed with prostate cancer who would be fit for curative treatment with PSA <10, PSA density <0.2, up to 2 biopsy cores positive with Gleason 3+3=6 cancer, and clinical stage T1c or T2. As of December 2010, patients aged 70+ with Gleason 3+4=7 were also made eligible for inclusion. End points to be assessed include continuation on active surveillance and clinical progression of prostate cancer. Results Twenty-six men have now been enrolledwith a median age of 63 (range 54 to 72). Baseline Information Twenty-three men were stage cT1c and 3 men were staged cT2a. On initial biopsy, 25 men had Gleason score 3+3=6 cancer and one man had a Gleason score 3+2=5 cancer. The median PSA was 6.0 ng/ml (range 0.9 to 9.2). The median follow up was 18 months (range 1 to 51 months). Outcomes At Follow Up 77% of men remain on active surveillance. 6 patients are no longer on active surveillance. 2 patients switched to watchful waiting due to development of significant co-morbidities, meaning they no longer required repeat biopsies and were no longer considered for curative treatment of prostate cancer. 2 patients were reclassified to more aggressive disease on repeat biopsy (Gleason score 6 to 7). These 2 patients both received seed brachytherapy 16 months after starting active surveillance due to evidence of disease progression as per protocol. The first patient was last followed up 5 months after brachytherapy with a PSA of 1.0 (from 1.1). The other patient was last followed up 15 months after brachytherapy with a PSA of 3.53. (from 6.1) 2 patients underwent radical prostatectomy. The first patient underwent a radical prostatectomy 23 months after starting active surveillance and was upstaged and upgraded from a cT1c tumour with Gleason score 3+3=6 to a pT3b tumour with seminal vesical invasion (clear margins) and Gleason score 3+4=7. At last follow up 6 months postoperatively his PSA was <0.05. The other patient underwent a radical prostatectomy 7 months after starting active surveillance and was upstaged and upgraded from a cT1c tumour with Gleason score 3+3=6 to a pT2c tumour with largely Gleason 3+3=6 and a small focus of Gleason 3+4=7 (clear margins). At last follow up 8 months after surgery his PSA was also undetectable. Data Entry Issues In our institution there was no data manager available so that data was directly added onto the PRIAS website by the clinician. Although data entry is straightforward and the website intuitive, ongoing entries for each follow-up visit became onerous and ideally requires the resource of a data manager. Aim We report on our involvement in this study to date. • Methods • After contacting the principal investigators in Rotterdam, fast-track ethics approval was obtained at our institution. Ethics approval was obtained in September 2009 and the first patient was enrolled later that month. Printed study information sheets and consent forms were made available in outpatient clinic rooms and eligible patients were invited to participate. Using a password, de-identified clinical data on each consenting patient were entered directly onto the PRIAS website by the clinician. No data manager was available. The follow-up protocol was then automatically displayed on the website for both patient and clinician to follow (Fig 1-2). Conclusions PRIAS is the largest ongoing study of men on active surveillance for prostate cancer. To date, our institution has accrued the largest number of patients in the Asia-Pacific region. The vast majority of this small cohort with short term follow-up remains on active surveillance. Enrolment and data entry was performed by the treating clinician. Whilst this was feasible, up-to-date data were difficult to maintain without additional resources. Involvement in this study of urologists in our region is encouraged. The recent provision by USANZ of the PRIAS data manager to assist urologists across Australia and New Zealand will facilitate accrual and is warmly welcomed. Fig 1. PRIAS follow up protocol References (1) Van den Bergh RCN, Roemeling S, Roobol MJ, Roobol W, Schroder FH, Bangma CH. Prospective Validation of Active Surveillance in Prostate Cancer: The PRIAS Study. European Urology. 2007;52:1560-1563. (2) ClinicalTrials.gov [Internet]: Canada: NCIC Clinical Trials Group; 2007. Identifier NCT00499174. A Phase III Study of Active Surveillance Therapy Against Radical Treatment in Patients Diagnosed With Favourable Risk Prostate Cancer [START]) [cited 1 Dec 2011]. Available from http://clinicaltrials.gov/ct2/show/NCT00499174. Poster presentation sponsor Fig 2. Screen shot of the website www.prias-project.org