Download
1 / 53
1.17k likes | 4.24k Views
Salivary Gland Disease. Dent 451 Lecture 6 Dr. Jumana Karasneh. Functions of Saliva. Lubricant coat & protect mucosa Cleanses the teeth Ion reservoir remineralization Buffer neutralizes PH Antimicrobial IgA & Enzymes Pellicle formation Digestion amylase

E N D
Salivary Gland Disease Dent 451 Lecture 6 Dr. Jumana Karasneh
Functions of Saliva • Lubricant coat & protect mucosa • Cleanses the teeth • Ion reservoir remineralization • Buffer neutralizes PH • Antimicrobial IgA & Enzymes • Pellicle formation • Digestion amylase • Facilitates taste by acting as solvent • Water balance stimulate need for fluid intake
Saliva • Resting salivary flow • Submandibular 65% • Parotid 15-20 % • Sublingual & minor 7-8 % • Stimulated salivary flow • Parotid (rich in amylase) 45-50% • Diurnal variation in salivary flow • 0.3 ml / min day time • 0.1 ml / min sleep time • Daily flow rate ~ 500-600 ml /day
Anatomy & Physiology • Parotid • Serous • Sublingual • Mucous • Submandibular • Mixed • Minor salivary glands • Controlled mainly by parasympathetic
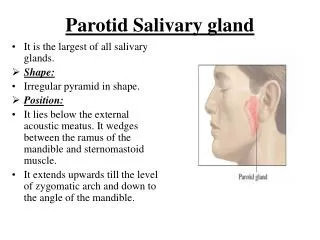
Anatomy of parotid gland • Largest salivary gland • Front of ear & behind mandibular ramus • Apex is deepest part • Facial nerve • Stenson’s duct covered by parotid papilla opposite second molar
Anatomy of submandibular gland • ½ the size of Parotid • Wedged between body of mandible & mylohyoid muscle • Wharton’s duct opens into sublingual papilla lateral to lingual frenum
Anatomy of sublingual gland • Smallest gland • Below floor of the mouth beneath sublingual fold • Numerous sublingual ducts open in the mouth
Assessment of the salivary gland1- Examination - Parotid • Visual examination by standing behind the Pt • Palpate the gland • Stand in front of pt • 2-3 fingers over the posterior border of ascending ramus • Back word & inward movement with light pressure • Slightly rubbery • Painless unless infected/inflamed • Check motor function of facial nerve • Intraoral examination to check papilla if inflamed • Compress the gland to see saliva flow
Assessment of the salivary gland1- Examination - submandibular • Palpate below angle & body of mandible • Bimanual palpation • Intraoral examination to check papilla if inflamed • Compress the gland to see saliva flow
Assessment of the salivary gland 2- Sialometry • To measure salivary flow rate (resting / stimulated) • Carlson-Crittenden collector for individual gland • Whole saliva flow rate determined under standardized conditions • Changes in salivary flow rate in an individual is more informative than a single measure • Unstimulated whole saliva flow rate ~ 0.3 ml/min • Stimulated whole saliva flow rate ~ 1-2 ml / min
Assessment of the salivary gland 3- Salivary gland imaging • Plain-film radiography • Sialography • Ultrasonography • Scintigraphy (Radioisotope imaging) • Computed tomography (CT) • Magnetic resonance (MRI)
Assessment of the salivary gland 3- Salivary gland imaging Plain-film radiography • Used for calculi (NOT ALL RADIO-OPAQUE) • Two views at 90 • Parotid • OPG / Oblique - lateral • Rotated anterior-posterior • Submandibular • Occlusal • OPG • Lateral oblique
Assessment of the salivary gland 3- Salivary gland imaging Sialography • Radiographic visualization of the ducts by a retrograde injection of a water-soluble contrast dye. • Provides image of stones* and duct morphological structure • May be therapeutic. • Demonstrate 3 phases: • Preoperatively • Filling phase • Emptying phase
Sialography continued… • Disadvantages: • Irradiation dose • High skill is needed to conduct the procedure • Pain with procedure • Possible perforation • Push stone further • Contraindications: • Acute infection • Calculus close to duct opening • Allergy to contrast media
Assessment of the salivary gland 3- Salivary gland imaging Scintigraphy (radioisotope) • Indications: To assess salivary gland function • Pass through 3 stages: • Flow phase 15-20 sec • Concentration phase up to 10-15 min • Symmetrical distribution in parotid, submandibular • Washout phase • Pt is given a lemon juice drop • Prompt, uniform & symmetric emptying
Assessment of the salivary gland 3- Salivary gland imaging Ultrasonography • Shows superficial part of gland • Indications: • Differentiate between extra & intra glandular mass • Differentiate between cystic & solid lesion Hypoechoic benign tumor Echogenic sialolith
Assessment of the salivary gland 3- Salivary gland imaging Magnetic resonance imaging (MRI) • Indications: • Suspected salivary gland tumour • Proximity of the lesion to facial nerve • Contraindications: • Paediatric cases • Claustrophobic • Mentally & physically challenged
Assessment of the salivary gland 3- Salivary gland imaging Computed tomography (CT) • Indications: • Sialolith • Osseous erosions & sclerosis • To differentiate cysts from abscess • CT Vs MRI
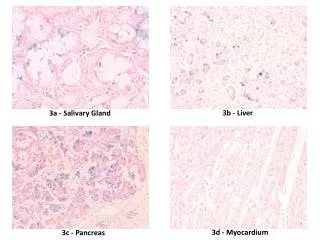
Assessment of the salivary gland 4- Salivary gland biopsy • Labial minor salivary gland biopsy • Sjögren’s syndrome • Amyloidosis • FNA • Major salivary gland mass • Major salivary gland biopsy • Extra-oral • High morbidity
Salivary Gland Disease Dent 451 Lecture 7 Dr. Jumana Karasneh
Specific diseases & disorders of salivary glands • Sialadenitis • Sialosis • Necrotizing sialometaplasia • Sarcoidosis • HIV- associated salivary gland disease • Salivary gland tumours • Disturbance of salivary flow • Xerostomia • Sjögren’s Syndrome
Sialadenitis • Inflammation of salivary gland • Bacterial • Viral (Mumps) • Allergic • irradiation • Usually affect major salivary glands but minor might be affected • Sjögren’s • Necotenic stomatitis Infective Non-infective
Bacterial sialadenitis • Usually secondary to localized or systemic predisposing factors • Reduction in salivary flow due to localized (calculus) or systemic casus (Sjögren’s) • Low immunity • Clinical picture: • Sudden onset (acute) • Gland is painful , swollen & indurated • Erythematous overlying skin • Purulent discharge from orifice • Chronic form might follow resolution of acute infection or start as chronic • Recurrence if inadequately treated or persistent predisposing factor
Bacterial sialadenitis • Treatment • Antibiotics after culture and sensitivity, if not possible use flucloxacillin 500mg (1x4x5-7d) • Milk the gland several times a day (not during acute phase) • Increase hydration & use of Sialogogue • Improve oral hygiene • Remove predisposing factor if possible (calculus) • Excision of severely damaged gland (chronic/ recurrent)
Allergic sialadenitis • Caused by drugs or allergens • Clinical presentation: • Acute salivary gland enlargement • Itching over the gland • With/without rash • Treatment • Self-limiting • Avoid allergen • hydration
Sialosis • Painless non-inflammatory, non-neoplastic swelling of salivary glands • Parotid is most commonly affected and commonly bilateral • Unknown mechanism • Histologically presented as hypertrophy of serous acini
Sialosis • Predisposing factors: • Drug induced (antirheumatic, idoine containing drugs, adrenergic) • Hormonal (Diabetes, acromegaly) • Nutritional deficiency induced by anorexia nervosa • Chronic alcoholism • Medication induced salivary dysfunction
Sialosis • Management: • Detailed drug history • Liver function test • Blood glucose level • Growth hormone level • CBC and full blood investigation
Necrotizing sialometaplasia • Benign changes in form of the cells taking a more squamous morphology • More common in males and smokers • Results from vasculitic phenomenon (ischaemia) leading to necrosis of minor salivary glands • Unknown etiology with reports of LA role • Self-limiting
Necrotizing sialometaplasia • Clinical presentation • Red nodule • Deep ulcer with rolled margin • Necrosis • Moderate dull pain • 6-8 weeks
Sarcoidosis • Chronic granulomatous disorder affecting several organs • Lungs • Skin • Eyes • Parotid glands • Severity and duration of disease varies • Saliva flow would be affected • Mild improvement noticed with steroid therapy
HIV-associated salivary gland disease • HIV patient usually develop salivary gland problems and xerostomia • Swelling of parotid might be caused by: • Sjogren-like condition • Kaposi’s sarcoma • Lymphoma • Viral infection • Chronic parotitis
Salivary gland tumors • Majority of tumors occur in the parotid, 10% in minor salivary gland • Most minor salivary gland tumors occur in the junction between hard and soft palate, 20% in the lip • WHO classification of salivary gland tumours • Benign Tumors • Pleomorphic adenoma • Malignant Tumors • Mucoepidermoid carcinoma • Adenoid cystic carcinoma
Salivary gland tumors • Pleomorphic adenoma: • Slowly growing • Firm consistency • Normal overlying mucosa • Painless and doesn’t ulcerate unless traumatized • Signs of malignancy: • Rapid aggressive growing • Ulceration • Usually nature of tumor is unpredictable biopsy diagnosis achieved by histological examination • Adenomas of minor salivary gland should be excised with safety margin
Disturbance of salivary flowXerostomia • Subjective feeling of oral dryness • Not associated with salivary hypofunction • Sensory or cognitive disorders • Pt usually complains of bad taste, abnormal sensation, burning mouth • Associated with salivary hypofunction • Need to investigate causes of hypofunction
Disturbance of salivary flowXerostomia - Causes of hypofunction: • Loss of secretory tissue (Sjogren’s, sarcoidosis) • Disturbance of secretory innervation • Xerogenic drugs • Neurological disease • Systemic factors • Renal disturbances • Endocrine disturbances (diabetes) • Sjogren’s syndrome • Radiation to head & neck • Radioactive iodine for thyroid cancer • Cognitive disorders (depression, anxiety) • Aging
Disturbance of salivary flowXerostomia Examples of Xerogenic drugs: • Antidepressants • Antihistamines • Decongestant • Antiparkinsonian agents • Tranquillizers and hypnotics • Anticholinergic • Antihypertensive drugs (Diuretics) • Appetite suppressants
Disturbance of salivary flowXerostomia - investigation History: • Does the amount of saliva in your mouth feel too little? Too much? Not notice it? • Does your mouth feel dry while eating? • Do you frequently sip liquids while eating? • Do you have difficulties swallowing food? Symptoms • Thirst • Difficulty eating, speaking, wearing denture • Need sips of water while eating • Burning sensation of mouth • Abnormal taste & halitosis • Cracked lips and soreness of corners of mouth
Disturbance of salivary flowXerostomia - investigation Signs • Dryness of oral mucosa • Tongue fissuring & lobulation • Oral candidosis – angular chelitis • Thick stringy saliva • Difficulty milking saliva • Dental caries and periodontal problems • Swollen salivary glands (infection / autoimmune sialadenitis)
Disturbance of salivary flowXerostomia - Management • Preventive therapy • Florid rinses & gel • Oral hygiene • Symptomatic treatment • Water • Artificial saliva • Avoid products containing sugar, alcohol • Vaseline ointment to relief cracking • Topical antifungal • Regular check ups • Salivary stimulation • Local / topical stimulation (detectable salivary gland function) • Chewing (flavoured, sugar free, xylitol) • Systemic stimulation (Pilocrpine HCl)
Sjögren’s syndrome • Chronic autoimmune disease destructing exocrine glands • Unknown etiology • 1SS= lacrimal & salivary gland dysfunction • 2SS= 1SS + connective tissue disease • More common in female (9:1) • Middle - Old age group
Primary SS - Clinical picture • Mostly parotid gland is affected • Persistent / intermittent gland enlargement • bilateral, non-tender, firm, and diffuse swelling • saliva and altered saliva composition • Check of any recent changes to the character of the glands (nodularity) • significantly increased risk of developing B-cell lymphoma • Keratoconjunctivitis sicca
Secondary SS - Clinical picture • Dryness of the skin & pruritis • Dry and persistent cough • >50% have arthralgia with or without arthritis • Dysphagia, nausea, dyspepsia, and epigastric pain • Peripheral & cranial neuropathy
Diagnostic Criteria • Ocular Symptoms (at least one) • Dry eyes >3 months? • Foreign body sensation in the eyes? • Oral Symptoms (at least one) • Dry mouth >3 months? • Recurrent or persistently swollen salivary glands? • Need liquids to swallow dry foods? • Ocular Signs(Schirmer test) • Oral Signs(at least one) • Unstimulated whole salivary flow (≤1.5 mL in 15 minutes) • Abnormal parotid sialography • Abnormal salivary scintigraphy • Histopathology (Lip biopsy showing focal lymphocytic sialoadenitis) • Autoantibodies (at least one) • Anti-SSA (Ro) • Anti-SSB (La)
Serologic evaluation for Sjögren’s syndrome • Antinuclear antibodies (80%) • Anti SS-A, anti SS-B (60%) • RF (Rheumatoid factor) • ESR
For a primary Sjögren’s syndrome diagnosis: • Any 4 of the 6 criteria, must include either item 4 (Histopathology) or 5 (Autoantibodies) • Any 3 of the 4 objective criteria (3, 4, 5, 6)
Sjögren’s syndrome - Management • Symptomatic • Systemic cholinergic (Pilocarpine) • 5mg TID/QID (should not exceed 30mg/day) • Follow up • If tumor is suspected • MRI & CT • Major gland biopsy • Referral
Sialorrhea (ptyalism) • Rare complaint caused by: • Hypersecretion • New intraoral prosthesis • Infected or ulcerative lesions • Neuromuscular dysfunction • Cerebral palsy, Parkinson’s disease & epilepsy • Decrease swallowing induces drooling • Infants • Pt with neuromuscular disease