Download
1 / 50
540 likes | 860 Views
Complications of Continuous-Flow Left Ventricular Assist Devices. Cheryl A. Abbas, PharmD Clinical Pharmacist Advanced Heart Failure and Heart Transplant Thomas Jefferson University Hospital. Objectives.

E N D
Complications of Continuous-Flow Left Ventricular Assist Devices Cheryl A. Abbas, PharmD Clinical Pharmacist Advanced Heart Failure and Heart Transplant Thomas Jefferson University Hospital
Objectives • Review the physiological effects of a continuous-flow left-ventricular assist device (CF-LVAD) • Understand the role of pharmacotherapy in the management of CF-LVADs • Evaluate clinical symptoms and device findings in the diagnosis of CF-LVAD complications • Describe the pharmacotherapy of device-related complications
Role of Mechanical Circulatory Support • Progression of heart failure leads to refractory treatments • ~250,000 of 7 million patients will develop advanced disease • Inotropic support survival rate of 10-30% at 1 year • Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) • Fifth annual report: 7,000 patients in the United States • Increase in implanting centers from ~109 to ~147 in January 2011 to 2012 Chetan PB. J Heart Lung Transplant 2014;33:667-674.
Left Ventricular Assist Devices (LVADs) • Implanted pump delivering blood from left ventricle to ascending aorta • Flow rate up to 10 liters per minute • Mean pressure of 100 mm HG • Continuous flow vs. pulsatile devices • Greater durability • Reduced size and weight • Silent operation • Improved quality of life
Continuous-flow Devices BTT = Bridge to Transplant DT = Destination Therapy Slaughter, MS. J Heart Lung Transplant 2010;29:S1-S39.
LVAD Candidacy • Patient assessment: • Appropriateness based on degree of illness • Heart Failure Survival Score; Seattle Heart Failure Score • Ability to undergo operative procedure • Adequate family/caregiver support for long-term success Slaughter, MS. J Heart Lung Transplant 2010;29:S1-S39.
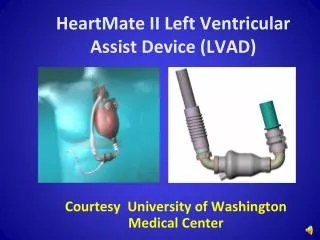
HeartMate II (HMII) • Rotary blood pump • Percutaneous driveline to external controller • External batteries or power-based unit • Estimated lifespan of pump: 5-10 years
CF-LVAD Physiology Slaughter, MS. N Engl J Med 2009;361:2241-51.
CF-LVAD Parameters • Speed: Fixed in range of 8,000 – 12,000 RPMs • Power: Direct measure of voltage to motor (4-7 watts) • Flow: Estimated speed x power (3-7 liters/minute) • Afterload sensitive - affected by hypertension • ↑AO → ↓Flow • ↓AO → ↑ Flow • Pulsatility Index (PI): Flow pulse through pump (4-8) • Native LV contractility and volume status Thoratec Press Kit: HMII Pivitol Trial Fact Sheet.
Blood Pressure Monitoring • Hemodynamic effect of CF-LVAD: Increase in diastolic pressure and flow • Reduced pulse pressure • Difficult to palpate pulse • Mean arterial blood pressure (MAP) measured by doppler • Goal MAP: 70-80 mmHG • Amount of cardiac output by CF-LVAD affected by afterload • Maintaining goal = optimized cardiac output • Reduces stroke due to hypertension
Blood Pressure Management • Vasoactive agents • ACEi/ARB, β-blockade, hydralazine, nitrates • Hypertension: assess BP and volume status • CF-LVAD parameters • Decrease in pump flow and power • Increase in PI • Management: Decrease afterload with medications • Consider diuretics for volume overload • Hypotension: symptoms, BP monitoring • CF-LVAD parameters • Increase in pump flow and power • Decrease in PI • Management: Adjust vasoactive agents • Intravascular fluid volume management Slaughter, MS. J Heart Lung Transplant 2010;29:S1-S39.
Anticoagulation • Required to avoid thrombotic complications • Early BTT HeartMate II trials included aggressive anticoagulation (AC) • Target INR range 2.5 to 3.5 • Incidence of thrombosis < bleeding resulted in reduced AC therapy • ISHLT MCS Guidelines • Anticoagulation: Warfarin with target INR based upon manufacturer • HeartMate II: 2.0 to 3.0 • Antiplatelet: Aspirin 81-325 mg daily in addition to warfarin • Additional agents may be added Feldman, D. J Heart Lung Transplant 2013;32:157-187.
Anticoagulation • Boyle, et al evaluated long term AC therapy in 331 HeartMate II outpatients • Risk of thrombosis increased with INR < 1.5 • Risk of hemorrhagic events present at all INR ranges; increased with INRs > 2.5 Slaughter, MS. J Heart Lung Transplant 2010;29:S1-S39.
Antiplatelet Agents • Increased platelet activation from sheer stress • Agents: • Aspirin 81-325 mg daily • Clopidogrel 7g mg daily • Dipyridamole 75 mg tid • Pentoxifylline 400 mg tid • Lack of data: Ticagrelor and Prasugrel • Hypo- or non-responsiveness is commonly seen • Doubling of dose
Patient Case • RW is a 63 y/o M PMH DM, HL, dilated NICM s/p LVAD placement (HMII) in 2014. He presents to clinic, where the LVAD coordinator obtains a doppler BP of 130 mmHG. When interrogating the device, what LVAD parameters may be found? A. Decreased PI B. Increased power C. Decreased flow D. None of the above
Pump Thrombosis • Development of clot within the flow path or any/all components • Leads to pump failure • Uncommon complication • ADVANCE trial 6.4% risk • HMII up to 6.25% risk • Pump-related risk factors: • Inflow cannula malposition • Outflow graft kink/compression • Low flows from low speeds or right-sided dysfunction Goldstein DJ, et al. J Heart Lung Transplant 2013;32:667–670. http://ejcts.oxfordjournals.org/content/39/3/414/F1.expansion.
Pump Thrombosis • Patient-related risk factors: • Atrial fibrillation • Pre-existent LV thrombus • Prosthetic mechanical valve • Sepsis • Sub-therapeutic INR • Inadequate anti-platelet therapy • Pro-coagulant states • Hemolysis is a result of shear stress!
Diagnosis of Pump Thrombosis • Routine diagnosis of hemolysis • Plasma Free Hemoglobin (pfHb) > 40 mg/dL • Lactate Dehydrogenase (LDH) > 3x ULN • Haptoglobin < 10 mg/dL • Dark red (tea-colored) urine • Power elevations (>10 watts) • Imaging • Chest x-ray and CT: malposition • Echocardiogram: suboptimal LV unloading • Right-heart catheterization: elevated pressures Goldstein DJ, et al. J Heart Lung Transplant 2013;32:667–670.
Treatment Options • Surgical: VAD exchange • Significant morbidity • Pharmacology • GPIIbIIIa inhibitors • Thrombolytics • Intraventricular vs peripheral administration • Modify antithrombotic therapy • Increase aspirin dose (81 to 325 mg daily) • Increase goal INR • Add antiplatelet agent (clopidogrel, dipyridamole)
Management of Pump Thrombosis Goldstein DJ, et al. J Heart Lung Transplant 2013;32:667–670.
Management of Pump Thrombosis • Retrospective review; single center, Jan 2006-Nov 2012 • Evidence of hemolysis + high clinical suspicion of VAD thrombosis, n=33 (of 217, 15.2%) • Mortality: 15/33, 45.5% • Treatment: (7 deaths) • Eptifibatide, n=9 • tPA, n=5 • Both, n=10 • No treatment, n=9 (5 pump exchanges, 4 deaths) • High mortality rate with and without pharmacologic treatment Lenneman AJ, et al. J Heart Lunt Translant2013; 32:S186-187.
Patient Case • CW is a 56 y/o F w/ICM s/p LVAD (HMII) who presented to the hospital from LVAD clinic with an increase in LDH to 764 (baseline 295) and persistent elevations in power >10 watts • PMH: CAD, sCHF with BiV ICD, COPD, DM • CW was started on IV heparin upon admission, and resumed her outpatient warfarin (goal INR 2-2.5) and aspirin 325mg qday
Patient Case Continued • Which of the following agents could be added to her anticoagulation regimen? A. Cilostazol 100mg po bid B. Clopidogrel 75mg poqday C. Dipyridamole 75mg potid D. B or C E. None of the above
Etiology • Most common adverse event after HMII • Incidence: 17-31% • Frequent and prolonged hospitalizations • Gastrointestinal angiodysplasia (GIAD) • Most common cause of GIB: 15-31% of total • Arteriovenous malformations (AVMs) • Gastric antral vascular ectasia (GAVE) • Retrospective, single-center review of 172 patients • 19% (32/172) rate of GIB • AVMs: 31% (10/32) Bunte MC, et al. J Am CollCardiol 2013;62:2188-96. Draper K, et al. J Heart Lung Transplant 2015;34(1):132-4.
Pathogenesis • Narrow pulse pressure:↓ intraluminal pressure • Vascular dilatation angiodysplasia, AVMs • Hypoperfusion intestinal mucosa ischemia • Over-expression of angiogenic growth factors • Acquired Von Willebrand Disease • Increased shear stress, turbulence, and high velocities • Von Willebrand factor cleavage increased bleeding and decreased platelet-mediated hemostasis
GIB: Patient Presentation • Decrease in hemoglobin (Hgb) • Obtain coagulation panel (PT/PTT/INR) • Symptoms: symptomatic anemia • Fatigue, dizziness, dyspnea on exertion • Melena • Hypotension (decreased MAP) • Adjust vasoactive medications • Decrease in PI • Consider volume expansion
Treatment Options • Blood transfusions to target Hgb • Problematic for patients listed for transplant • Addition of proton pump inhibitor • Prophylaxis vs. treatment • Colonoscopy +/- endoscopy: suspected bleeding sites • Endoscopic ablation of AVMs • Mechanical clipping • Cauterization • Argon plasma coagulation (APC) • Surgical resection Ray R, et al. ASAIO Journal 2014;60:482-483.
Modification of Current Therapy • Cessation of anticoagulation • Hold warfarin in setting of clinically significant bleed • Assess need for IV heparin when INR < goal • Reduction of anticoagulation • Decrease goal INR • Modify or discontinue antiplatelet therapy • Reduction of CF-LVAD speed • Increase pulse pressure reduce shear stress
Additional Therapies • Anticoagulation protocols • Reductions in response to bleeding • Octreotide • Difficult to tolerate: mode of delivery (injection) • Adverse effects: nausea and bradycardia • Thalidomide: potent anti-angiogenic compount • Inhibition of vascular endothelial growth factor (VEGF) • Recurrent GIAD-related bleeding • Associated thrombosis • REMS program • Lenalidomide: synthetic analog of thalidomide • Less non-hematologic adverse effects Draper K, et al. J Heart Lung Transplant 2015;34(1):132-4.
Preventative Strategies? • Additional studies needed: • Blood product use • Platelet aggregometry • Thromboelastography • Use is currently insufficient to make recommendations • Perioperative bleeding risk stratification • Individualized bleeding score • Could offer tailored post-operative AC to limit bleeding
Patient Case • JH is a 67 y/o M w/ICM s/p DT LVAD (HMII) implant in May 2015, p/w 2 episodes of melena overnight, dizziness, and fatigue. MAP on admission is 55 mmHG. LVAD interrogation shows multiple PI events (decreased). • Labs on admission: • Hgb 7.5 mg/dL (baseline 10.0 mg/dL) • INR 3.3 (goal INR 2-2.5) • Current medications: • Amiodarone 200 mg poqday, aspirin 325 mg poqday, carvedilol 12.5 mg po bid, furosemide 20 mg poqday, pantoprazole 40 mg poqday, potassium chloride 20 mEqpoqday, warfarin 5 mg poqday
Patient Case Continued • JH was transfused 2 units of PRBC and Gastroenterology was consulted with plan for colonoscopy for ? lower GIB. In addition to holding warfarin, what other medication adjustments would you make at this time? A. Discontinue furosemide 20 mg poqday B. Discontinue carvedilol 25 mg po bid C. Lower aspirin to 81 mg poqday D. All of the above
Epidemiology • CF-LVADs decreased rate of infection by 50% • Goldstein, et al. INTERMACS registry: • 2008-2013 implants; n = 9,372 • 2nd most common cause of death post 6-month survival • Most common: • Sepsis = 23% • Pneumonia = 20% • Percutaneous site/driveline infection (PSI) = 19% • Causative organisms • Staphylococcus species • Pseudomonas species • Prominent w/longer VAD support • Difficult to eradicate Goldstein DJ, et al. J Heart Lung Transplant 2012;31(11):1151-7.
Complications of Infection • Association with cerebrovascular events (CVEs) • Persistence of bacteremia > 72 hours • Persistent Pseudomonas aeruginosa blood stream infections 7-fold increase in CVEs • Mycotic aneurysms • Potential mechanisms of CVEs: • Platelet activation • Alterations in endothelial function • Systemic inflammation • Bacterial seeding of cerebral vasculature Aggarwal A, et al. ASAIO J 2012;94(5):1381-6.
Pathophysiology • Disruption or trauma to the barrier between skin and driveline • Formation of biofilm • Increase difficulty to eradicate bacteria • Staphylococcus and Pseudomonas • Peri-operatively and post-operatively • Average time to occurrence of PSI = ~6 months • PSI locations • May remain superficial • Spread along driveline path, into pocket or pump • Deepen within abdominal wall to form abscess Trachtenberg B, et al. MDCVJ 2015;11(1):28-32.
Classification of Infection CVC: central venous catheter BSI: blood stream infection SSI: surgical site infection Trachtenberg B, et al. MDCVJ 2015;11(1):28-32.
Prevention • Immobilization of percutaneous lead at exit site • Prevents disruption of subcutaneous tissue growth • Methods: minimize trauma and tension • Anchoring devices • Stabilization belts • Exercise sterile vs. clean technique for exit site care • Patient education • Report increased drainage or erythema immediately • Gentle and non-traumatic exit site cleaning
Prevention: Perioperative Antibiotics • REMATCH study (HeartMate XVE): • Vancomycin 15 mg/kg IV 1 hour pre-op then q12h • Levofloxacin 500 mg IV 1 hour pre-op then q24h • Rifampin 600 mg po 1 hour pre-op then q24h • Fluconazole 200 mg IV 2 hours pre-op then q24h • Most centers omit rifampin, use β-lactams, or tailor to institutional antibiogram • Continue for 48-hours • HeartWare recommendations: • Cover S. aureus, S. epidermidis, and Enterococcus according to institutional antibiogram Richenbacher WE, et al. Ann ThoracSurg2003;75:S86-92.
Diagnosis • Prompt culture of drainage • 3 sets of blood cultures • Imaging • Chest radiography • Echocardiogram: pacemakers or defibrillator leads • Presence of valvular endocarditis or device infections • Ultrasound or CT: • Diagnose collections of fluid around driveline, pump, or pump pocket • Guide aspiration or debridement Feldman D, et al. J Heart Lung Transplant 2013;32(2):157-87.
Treatment Options • Hospitalization criteria: • Signs of systemic infection = fever or leukocytosis • Mild infection: • Increase frequency of dressing changes • Review dressing change protocols for compliance • Moderate infection: • Tailor antibiotic therapy • Local debridement • Weekly clinic visits • Severe infection: purulent drainage and subcutaneous induration • Target antimicrobial therapy with ID consult • Imaging tests • Surgical interventions: debridement or retunneling of driveline Trachtenberg B, et al. MDCVJ 2015;11(1):28-32.
Treatment Options • Additional tools • Wound vacuum-assisted closure therapy • Antimicrobial beads • Chronic suppressive oral antibiotics • For recurrent VAD-specific or VAD-related infections • 1/3 of patients have recurrence despite antibiotics • Device exchange (severe cases) • Expediting heart transplant listing • Studies show no increase in mortality post-transplant
Overview: CF-LVAD Complications • Newer devices improvements in survival • Every VAD patient is different! • Importance of understanding VAD-specific parameters • Balancing act between VAD thrombus and GIB • Preventative measures of infection • Need more data • Publish your experience!!!