Download
1 / 50
500 likes | 702 Views
神经系统病理. Diseases of the Nervous System. Fangying Xu xfy@zju.edu.cn. 感染性疾病. 感染途径 血源性感染:脓毒血症 局部扩散:如中耳炎 直接感染:如创伤或医源性 经神经感染:单纯疱疹病毒沿三叉神经入侵 细菌性疾病 病毒性疾病 海绵状脑病. 细菌性疾病. 脑脓肿 (brain abscess) 脑膜炎 (meningitis) 硬脑膜炎 (pachymeningitis) :继发于颅内感染 软脑膜炎 (leptomeningitis) :

E N D
神经系统病理 Diseases of the Nervous System Fangying Xu xfy@zju.edu.cn
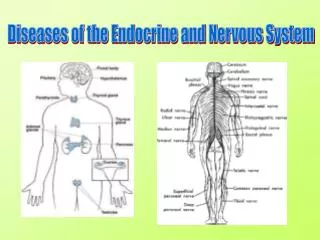
感染性疾病 感染途径 • 血源性感染:脓毒血症 • 局部扩散:如中耳炎 • 直接感染:如创伤或医源性 • 经神经感染:单纯疱疹病毒沿三叉神经入侵 • 细菌性疾病 • 病毒性疾病 • 海绵状脑病
细菌性疾病 • 脑脓肿(brain abscess) • 脑膜炎(meningitis) 硬脑膜炎(pachymeningitis):继发于颅内感染 软脑膜炎(leptomeningitis): 蛛网膜、软脑膜及脑脊液的感染 化脓性脑膜炎:细菌为主 淋巴细胞性脑膜炎:病毒感染 慢性肉芽肿性脑膜炎:由结核杆菌等引起
EPIDEMIC CEREBROSPINAL MENIGITIS (流行性脑脊髓膜炎) Definition: Acute purulent inflammation of leptomeningitis, subarachnoid space and the spinal meninges caused by meningococcus(脑膜炎双球菌, Neisseria meningitidis)
Etiology Generally, pyogenic meningitis may be caused by Meningococcus(脑膜双球菌), pneumococci(肺炎双球菌), streptococci(链球菌), Staphylococci(葡萄球菌), influenza bacilli(流感细菌), actinomyces(放线菌), and rarely, colon bacilli in infants. The most important of these is the meningococcus.
脑膜炎双球菌(学名Neisseria meningitidis),又名脑膜炎奈瑟菌或脑脊髓膜炎双球菌,简称为脑膜炎球菌,是一种革兰氏阴性菌,1887年Weichselbaum首次从脑脊液中分离出 • 内毒素 • 细菌表面成分 • 菌毛:粘附器 • 感染性强,但对外界的抵抗力较弱,存活能力差。本菌含自溶酶,如不及时接种易溶解死亡 • 对寒冷、干燥较敏感,低于35℃、加温至50℃或一般的消毒剂即可杀死
Epidemic features Source of infection: Patient in disease Pathogen carrier without symptoms 50% in normal persons could be found with Neisseria meningitidis in epidemic season. Route of transmission: Air transmission, e.g. by cough, sneezing Intimate touch, e.g. kiss, breast-feeding Susceptible population: 6 months old –2 years old in peak susceptible population. Epidemic season: most in spring and winter
Pathogenesis (上呼吸道感染期) (败血症)期 (脑脊髓膜炎期) (化脓性脑膜炎) (沃-弗综合征)
A. Pathological features of purulent meningitis Morphology Grossly: An exudate is evident within the leptomeninges over the surface of the brain. The meningeal vessels are engorged and stand out prominently.
软脑膜及蛛网膜下腔可见大量脓性渗出物,血管扩张充血软脑膜及蛛网膜下腔可见大量脓性渗出物,血管扩张充血
Microscopically The subarachnoid space contains purulent exudates with varying amounts of fibrin. In most severe cases, the entire subarachnoid space is filled with purulent exudates. In less severely affected cases, only the tissue around the leptomeningeal blood vessels contains cells.
蛛网膜下腔间隙增宽,毛细血管扩张,大量炎性渗出物积聚蛛网膜下腔间隙增宽,毛细血管扩张,大量炎性渗出物积聚
炎性渗出物以大量中性粒细胞和纤维蛋白渗出为主及少量淋巴细胞、单核细胞浸润炎性渗出物以大量中性粒细胞和纤维蛋白渗出为主及少量淋巴细胞、单核细胞浸润
B. Pathological features of fulminant meningitis In fulminant infections, apparent sepsis symptom and signs appear with the less severely purulent exudates around the leptomeningeal and subarachnoid space, even without meningeal inflammation. Fulminant meningitis could be divided into: Shock type and meningitis-encephalitis type
Pathological features of fulminant meningitis 1. Shock type: Waterhouse Friderichsen syndrome(沃-弗综合征):两侧肾上腺 严重出血,肾上腺皮质功能衰竭,表现为周围循环衰竭、休克 和皮肤大片紫癜。 机制:大量内毒素释放引起的DIC A group of shock symptoms: High fever and chill Headache and vomiting Skin eruption ( petechia and ecchymosis) The cold extremities and paleness Weak pulse and low pressure DIC (disseminated intravascular coagulation)
Pathological features of fulminant meningitis 2. Meningitis-encephalitis type 脑膜脑炎 A group of symptoms involving damages of central nervous system accompanied with the tri-signs in infectious diseases: heavy headache, high pyrexia and vomiting 脑实质损害的临床症状明显 患者迅速进入昏迷,嗜睡,惊厥频繁 锥体束征常阳性,两侧反射不等 血压持续升高,眼底可见视乳头水肿 部分病人发展为脑疝 瞳孔明显缩小或散大,或忽大忽小
Clinicopathologic association 1)Signs of meningeal irritation(脑膜刺激症状) 2)Increased intracranial pressure(颅内压升高症状) 3)Changes of cerebrospinal fluid (CSF)(脑脊液改变)
Clinicopathologic association 1)Signs of meningeal irritation Heavy headache Opisthotonus(角弓反征) Kernig sign+(屈髋伸膝征阳性) Stiff neck(颈项强直) Clouding of consciousness
Clinicopathologic association 2) Increased intracranial pressure 头痛、喷射性呕吐、脑疝形成、小儿前囟饱满 Some degree of acute internal hydrocephalus results from an increased permeability of the choroids plexus, an outpouring of exudates into the ventricular. This condition, along with edema, congestion of blood vessels, and subarachnoid exudates, increases the intracranial pressure, which causes tri-signs in intracranial pressure: heavy headache and dizziness, jetting-vomiting and hernia formation 侧卧位脑脊液压超过2.0Kpa(正常:0.6-0.8Kpa)
In fulminant infection, bacteria may sometimes be visible on smear or be readily cultured for a few hours before polymorphos appear.
结局和并发症 • 脑积水 • 脑神经受损麻痹:III,IV,V(三叉神经),VI(展神经)和VII(面神经) 动眼神经(III)麻痹表现为上睑下垂,眼球外斜,向上外、上内、下内、同侧方向运动障碍,瞳孔散大,对光反应及调节反应消失 滑车神经(IV)麻痹表现为眼球不能向下外方向运动,伴有复视,头呈特殊位,呈下颏向下头面向健侧的姿势 • 脑缺血和梗死
病毒性疾病 80%以上的中枢神经系统病毒感染是由肠道病毒(enteroviruses)引起的 包括柯萨奇病毒(Coxsackie virus)、埃可病毒(ECHO virus)、 脊髓灰质炎病毒(polio-virus)等 其次是疱疹病毒(herpes virus),水痘-带状疱疹病毒(varicella-zoster virus) 巨细胞病毒(cytomegalovirus,CMV)等 呼吸道病毒(respiratory virus)、麻疹病毒(measles virus) 风疹病毒(rubella virus) 、狂犬病病毒(rabies virus)、腮腺炎病毒 (mumps virus) 和虫媒病毒等也可引起 www.themegallery.com
中枢神经系统病毒感染的特点: • 绝对细胞内寄生:不同病毒定位于不同细胞或核团 疱疹病毒:颞叶及顶叶眶部 • 病毒感染的细胞出现:细胞溶解、小胶质细胞增生形成结节、多核巨细胞形成 包涵体:胞质或胞核中,狂犬病毒时的Negri小体 • 炎症细胞以淋巴细胞、巨噬细胞和浆细胞为主,形成袖套现象(vascular cuffing)
Type B Epidemic Encephalitis(流行性乙型脑炎) • 乙型脑炎病毒感染所致的急性传染病,多在夏秋季流行 • 高热、嗜睡、抽搐、昏迷等 • 10岁以下儿童多见,约占50-70% • 全国乙脑报告病例数每年在5000~10000例之间,但局部地区时有暴发或流行。而全世界病例数每年高达50000例,死亡数15000例
Etiology A great many viruses may cause epidemic encephalitis. In China, India, Southeast Asia and Korea, as well as Japan, epidemic encephalitis is caused be a flavirus(黄病毒), Japanese encephalitis virus. • In order to distinguish it from von Economo’s(A) type encephalitis, it was named Japanese encephalitis B or epidemic encephalitis B • 乙型脑炎病毒属披膜病毒科黄病毒属第1亚群,呈球形,直径20~40nm • 为单股RNA病毒
Epidemics Sources of infection Route of transmission Susceptible population Epidemic season Pigs, cows, sheep, dogs, chicken, duck and goose infected Vector: mosquito [库蚊(Culex)、伊蚊(Aedes)和按蚊(Anopheles)] It has a seasonal incidence and mosquito vector, mainly occurring in summer and often affecting the children (most of 2- 7years of age).
Morphology • Mainly involves cerebrospinal parenchyma • Gross appearance: softening area in cerebral parenchyma, especially in cortical 粟粒或针尖大小的半透明软化灶 皮质深层、基底核、视丘等处最严重,其次是小脑皮质、延髓及脑桥,脊髓病变最轻
Morphology Microscopically: Degeneration and necrosis of neurocyte(神经细胞变性坏死) Softening area formation(软化灶形成) • Perivascular inflammatory cell infiltration(脑血管改变) • Proliferation of microgliacyte(胶质细胞增生)
Microscopically 1. Degeneration and necrosis of neurons: Neuronophagia phenomenon (噬神经细胞现象 ): individual neuron necrosis and phagocytosis by microglial cells. 小胶质细胞或血源性巨噬细胞包围吞噬坏死神经元后,可形成泡沫细胞或格子细胞 Satellite phenomenon(神经细胞卫星现象): 1个神经元由5个或以上少突胶质细胞(oligodendrocyte)围绕
Necrosis of neurons 神经元肿胀、尼氏小体消失、胞质内空泡形成、核偏位或固缩/溶解/消失
2. Softening area formation: Focal neuronal necrosis and show a loose ,light-stain sieve structure 软化灶:灶性神经组织坏死、液化形成镂空状筛网状结构 具诊断价值
3. Perivascular inflammatory cell infiltration The most characteristic histological change in acute viral disease is a mononuclear cell infiltrate (lymphocytes, plasma cells, and macrophages), generally located around blood vessels (perivascular cuffing).
血管扩张,周围间隙增宽,浸润的炎症细胞形成血管套血管扩张,周围间隙增宽,浸润的炎症细胞形成血管套
4. Proliferation of microgliacyte: Microglial nodules. The presence of glialnodules and neuronophagia (individual neuron necrosis and phagocytosis) also suggests viral disease. 另外 ,少突胶质细胞增生明显 星形胶质细胞增生和胶质瘢痕形成
小胶质细胞结节 The presence of glialnodules
The clinical Courses 最早和主要的症状:嗜睡、昏迷 脑神经麻痹症状 脑水肿和颅内压升高 脑疝(brain hernia):小脑扁桃体疝 脑膜刺激征 实验室检查 外周血检测: 白细胞总数常在1万~2万/mm3,中性粒细胞在80%以上 脑脊液:无色透明,压力仅轻度增高,白细胞计数增加,病初2~3天以中性粒细胞为主,以后则单核细胞增多为主。糖正常或偏高,蛋白质常轻度增高
结局: • 急性期痊愈 • 数月后恢复正常 • 后遗症:痴呆、语言障碍、肢体瘫痪等