Download
1 / 33
330 likes | 508 Views
Duchenne Muscular Dystrophy in Adults. Dr Emma Husbands Consultant Palliative Medicine GHNHSFT. Overview of Duchenne Issues in transition What can adult Pall Care offer?. Muscular dystrophies.

E N D
DuchenneMuscular Dystrophyin Adults Dr Emma Husbands Consultant Palliative Medicine GHNHSFT
Overview of Duchenne • Issues in transition • What can adult Pall Care offer?
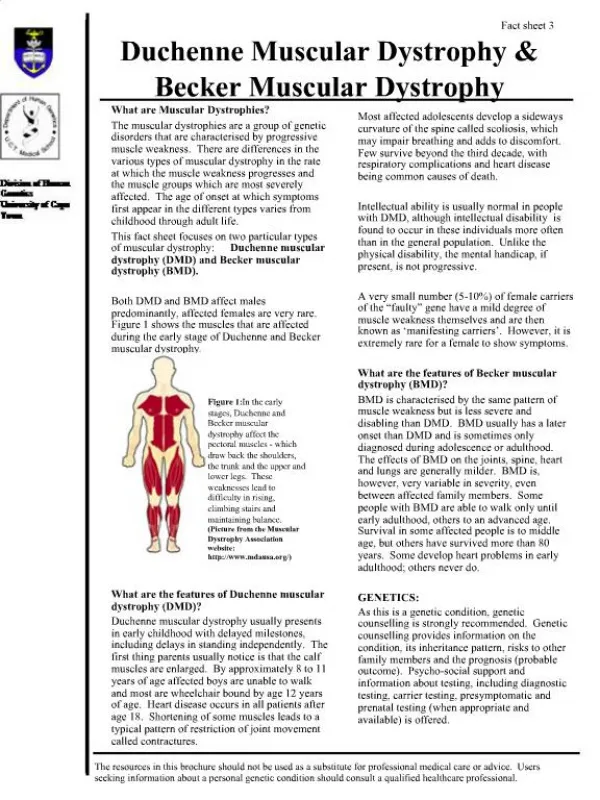
Muscular dystrophies • Group of muscle diseases characterized by progressive weakness, defects in muscle proteins, and the death of muscle cells • 1860’s Guillaume Duchenne described boys who grew progressively weaker and died in their teens. • Named after him • It soon became evident that the disease had more than one form. • Now over 50
DMD Facts • DMD affects mostly males at a rate of 1 in 3,500 births. • 100 boys w/ DMD are born in the United Kingdom each year. • There are about 1500 known boys w/ the disorder living in the UK at one time. • 60% inherited • X-linked recessive • 1/3 have family history • 30% spontaneous mutation • Most severe and common type of muscular dystrophy.
DMD is characterized by the wasting away of muscles. • Due to deficiency of the muscle protein Dystrophin • Diagnosis in boys usually occurs between 16 months and 8 years. • Parents are usually the first to notice problem. • Without intervention, average age survival 19yrs • Improved use of respiratory support can see survival into 40’s
Clinical Features • Increase in serum CK (creatine phosphokinase) levels up to 10 times normal amounts. • Wheelchair bound by 12 years of age. • Scoliosis common • Cardiomyopathy at 14-18 years. • Respiratory problems lates teens onwards • Scoliosis may exacerbate this
Corticosteroids Respiratory Support NIPPV Cough assist Trachaeostomy ACE-Inhibitors, Beta blockers Spinal Surgery Nutritional support Exercise Gene therapy……. Improvements in Prognosis
Problems for Adults • Cramps/spasticity • Magnesium supplements/quinine/G&T • Respiratory problems • Likely on NIPPV or approaching it • Potential consideration for trachae – implications for care • Cardiac arrhythmias • Continue ACE-Inhibitors/Beta Blockers • Swallowing difficulties • May have/need PEG • Could try prokinetics
Increased incidence of mental health issues • Low mood/depression • Anger/frustration • Desire for normality • Learning difficulties in 5% of patients. • Verbal memory can be impaired, possibly exacerbated by hypercapnoea • Disengagement with medical services by families is not uncommon
Family pressures • Care often falls to parents • Young men may want/struggle to achieve independence • Life will be limited Warrant a holistic approach
With increasing survivorship, now entering adulthood and less practical to remain under paeds services • Can be a sense of abandonment when entering the adult healthcare word…… • One paediatrician their whole life
Why Get Us Involved? • Neurology support often time-limited and possibly regional • Locally, we can provide a specialist link which can react as needed • Condition remains life-limiting • just a bit less limiting than before • Practical care needs • Respite services are lost • Supportive care needs…………… • Patient • Family • Advance care planning needs……
J • 17yrs old DMD • Admitted to adult resp ward with chest infection, type 2 resp failure • Also c/o reflux/nausea/constipation • Often missed OPA’s as a kid • Known LV dysfunction, non compliant with ACE -Inhibitors • Referral from team to explore discharge planning
On ward, family present 24/7 • Parents clear on admission, J present • Do not want active intervention – requested DNACPR, no to ICU • Paeds cons popped to say hello to patient on their own • J not sure about DNACPR – paeds cons revoked and suggested discussion held – left that to us!!!!!! • WHO’s CHOICE? • WHAT CHOICE?
THE ICPCN CHARTER OF RIGHTS FOR LIFE LIMITEDAND LIFE THREATENED CHILDREN The child’s parents or legal guardians shall be acknowledged as the primary care givers and recognised as full partners in all care and decisions involving their child. Every child shall be encouraged to participate in decisions affecting his or her care, according to age and understanding. The child and the family shall be given the opportunity to consult with a paediatric specialist with particular knowledge of the child’s condition where possible, and shall remain under the care of a paediatrician or doctor with paediatric knowledge and experience.
The child and the family shall be entitled to a named and accessible key-worker whose task it is to build, co-ordinate and maintain appropriate support systems which should include a multi-disciplinary care team and appropriate community resources. The child’s home shall remain the centre of care whenever possible. Treatment outside of this home shall be in a child-centred environment by staff and volunteers, trained in palliative care of children. Every child and family member, including siblings, shall receive culturally appropriate, clinical, emotional, psychosocial and spiritual support in order to meet their particular needs. Bereavement support for the child’s family shall be available for as long as it is required.
ACP in Transitional Population Parents will protect their children Hard for them, they may be used to being in control Reality checks over what is on offer Young people with MD have different life experience And remember they are teenagers Want ‘normality’ and independence Sex and drugs and rock and roll Fears they cannot mention to parents Meeting young adults in a crisis is not great Constant discussions/building relationships
Analysis of an adult Duchenne muscular dystrophy populationA.E. PARKER1, S.A. ROBB, J. CHAMBERS, A.C et al. Q J Med 2005; 98:729–736 • Patients rarely wished to discuss the later stages of their disease. • Death was often more precipitate than expected • In some, there was a clear progressive deterioration of ventilatory function. • Death usually occurred outside hospital.
J CPR was medically not indicated given reserves and overall decline The outstanding issue was option for trachae Agreed J would not want to ‘wake-up’ with a trachae on ICU Did not rule out option for planned procedure We also tweeked his meds Erythromycin 250mg bd for gastric prokinesis to aid reflux and bowels PRN oramorph, buccal midazolam Parenteral meds available
Went home with NIPPV • ACP in place, OOH alerts, anticipatory meds • At college so needed liaison with them • Settled period of several months • One DV, t/c f/u • Case conference at college due to absences • No admissions • Then acute decline, mum felt J dying, paeds hospice team supported, happy for me to review, arranged but died day before seen peacefully at home, on NIPPV.
Remove NIPPV • Sudden death common • If the norm for patient does it matter to die on NIPPV? • Not routine to discuss planned discontinuation • If request to remove • Plan • Ensure adequate sedation to avoid distress • Likely IV, pall med team might be able to help with this is community
C 22yr old DMD Had been a late diagnosis family felt they had always done the leg-work Parents very wary of our involvement Minimal symptoms Main issues Keen to do stuff Linking in with Douglas House Should he exercise? If so where/how? Would be happy for hospital admission if needed but pleased with reviews at home
Becoming an adulthttp://www.bristol.ac.uk/norahfry/research/completed-projects/becominganadult.pdf • Qualitative study focussing on what it’s like to live with Duchenne and become an adult. • Interviews throughout 2007 and 2008, involved 40 young men aged 15 to 33 who have Duchenne (and their families) from three regions of England – West Midlands, South West and North East.
Living with Duchenne can be a hard thing to talk about. “In everyday life I don’t think about it much.” “Sometimes you talk about it and sometimes you don’t. I’m not bothered about talking about it though.” “I live with it everyday. I know what I need to know. I’m not really interested.” • When people did want to talk about it, they usually talked to parents or friends but it wasn’t always easy. Some people said it was hard to talk to their parents because they wanted to protect them; they didn’t want their parents to get upset.
“I said I didn’t want to see lots of different doctors all the time. The last thing I want is seeing a load of doctors who depress me with bad news! But I thought I’d better see someone, so I asked who would be the most use and I went for the respiratory consultant.” • “You need continuity and you need a person who you can be friends with before you’re going to tell them things.”
(Soanes & Timmons, 2004; ACT et al, 2001). • Young people need: • continuity and familiarity • to be prepared for change • any new service to be flexible and account for individuality • good quality support along with staff showing that they care (with kindness, or understanding, for example).
C • Explained what advance care planning is but not covered it • Put in touch with specialist OT • Found some ‘adventure’ holiday options • Email contact given • Reviewing 3mthly
What I have learnt so far….. • One size will not fit all • If verbal processing is difficult, we may need to alter formats of discussion. • Not simply young adults • Different life experience • Families cannot be removed • Building a rapport is often key • Parents add another dimension!
As ever, emphasis on education • around what our role is • Referral may be for advance care planning but this may not be what is needed/addressed • around the advances in Duchene for adult physicians
Joint clinics with paeds? • Community aspect of our role helps • Neuromuscular co-ordinators invaluable • Specialised commissioning will hopefully improve access to cough assist etc • MDT working – what we do best!