Download
1 / 1
10 likes | 119 Views
Spatial Patterns in CBF Depression in Alzheimer’s Disease from Multi-variate Analysis of Continuous Arterial Spin Labeling MR Truman R. Brown 1 , Christian Habeck 2 , Ajna Borogovac 1 , Nikolaos Scarmeas 2 Yaakov Stern 2 , Iris Asllani 1

E N D
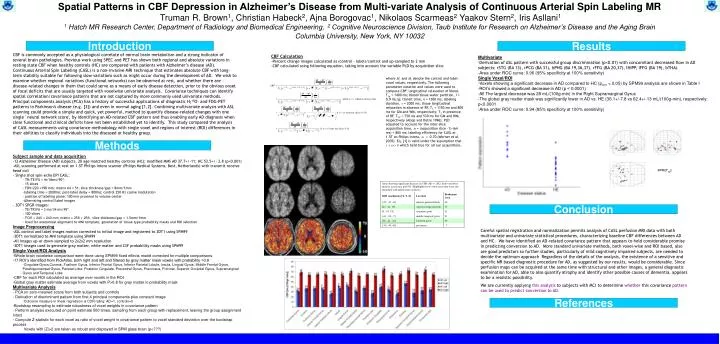
Spatial Patterns in CBF Depression in Alzheimer’s Disease from Multi-variate Analysis of Continuous Arterial Spin Labeling MR Truman R. Brown1, Christian Habeck2, Ajna Borogovac1, Nikolaos Scarmeas2 Yaakov Stern2, Iris Asllani1 1 Hatch MR Research Center, Department of Radiology and Biomedical Engineering, 2 Cognitive Neuroscience Division, Taub Institute for Research on Alzheimer’s Disease and the Aging Brain Columbia University, New York, NY 10032 Introduction Results • CBF Calculation • Percent change images calculated as (control – label)/control and up-sampled to 2 mm • CBF calculated using following equation, taking into account the variable PLD by acquisition slice CBF is commonly accepted as a physiological correlate of normal brain metabolism and a strong indicator of several brain pathologies. Previous work using SPEC and PET has shown both regional and absolute variations in resting state CBF when healthy controls (HC) are compared with patients with Alzheimer’s disease (AD). Continuous Arterial Spin Labeling (CASL) is a non-invasive MRI technique that estimates absolute CBF with long-term stability suitable for following slow variations such as might occur during the development of AD. We wish to examine whether regional variations (functional networks) can be observed at rest, and whether there are disease-related changes in them that could serve as a means of early disease detection, prior to the obvious onset of focal deficits that are usually targeted with voxelwise univariate analysis. Covariancetechniques can identify spatial correlation/covariance patternsthat are not captured by more commonly used univariate methods. Principal components analysis (PCA) has a history of successful applications of diagnostic H215O- and FDG-PET patterns in Parkinson's disease (e.g. [3]) and even in normal aging [1,2]. Combining multivariate analysis with ASL scanning could provide a simple and quick, yet powerful, method to quantify disease-related changes with one single ' neural network score', by identifying an AD-related CBF pattern and thus enabling early AD diagnosis when clear functional and clinical deficits have not been established yet to identify. This study compared the analysis of CASL measurements using covariance methodology with single voxel and regions of interest (ROI) differences in their abilities to classify individuals into the diseased or healthy group. • Multivariate • Derivation of ASL pattern with successful group discrimination (p<0.01) with concomitant decreased flow in AD subjects: rSTG (BA 13), rPCG (BA 31), bPHG (BA 19,36,37), rFFG (BA 20,37), lHIPP, lFFG (BA 19), bTHAL • Area under ROC curve: 0.96 (95% specificity at 100% sensitivity) • Single Voxel/ROI • Voxels showing a significant decrease in AD compared to HC (pcorr < 0.05) by SPM99 analysis are shown in Table I • ROI’s showed a significant decrease in AD (p < 0.0001) • All The largest decrease was 28 mL/(100g-min) in the Right Supramarginal Gyrus • The global gray matter mask was significantly lower in AD vs. HE (36.1+/-7.8 vs 62.4+/-13 mL/(100g-min), respectively; p<0.0001 • Area under ROC curve: 0.94 (85% specificity at 100% sensitivity) where Mc and Ml denote the control and label voxel values, respectively. The following parameter notation and values were used to compute CBF: longitudinal relaxation of blood, T1a = 1400 ms; blood/tissue water partition, l = 0.9 mL/g; transit time, d = 1300 ms; labeling duration, t = 2000 ms; tissue longitudinal relaxation in absence of RF, T1 = 1150 ms and 800 ms for GM and WM, respectively; T1 in presence of RF, T1rf = 750 ms and 530 ms for GM and WM, respectively (Alsop and Detre 1996); PLD adjusted to account for the inter-slice acquisition time, w = (acquisition slice –1)·(64 ms) + 800 ms; labeling efficiency for CASL at 1.5T on Philips Intera, a = 0.70 (Werner et al. 2005). Eq. [1] is valid under the assumption that t + w > d which held true for all our acquisitions. Methods • Subject sample and data acquisition • 12 Alzheimer Disease (AD) subjects, 20 age matched healthy controls (HC); modified MMS AD 37.7+/-11; HC 53.5+/- 2.8 (p<0.001) • ASL scanning performed at rest on 1.5T Philips Intera scanner (Philips Medical Systems, Best, Netherlands) with transmit-receive head coil • Single shot spin-echo EPI CASL: • TR/TE/FA = 4s/36ms/90º; • 15 slices • FOV=220 ×198 mm; matrix 64 × 51; slice thickness/gap = 8mm/1mm • labeling time = 2000ms; post-label delay = 800ms; control 250 Hz cosine modulation • position of labeling plane: 100 mm proximal to volume center • Alternating control/label images • 3DT1 SPGR images: • TE/TR/FA = 3 ms/34 ms/45º • 100 slices • FOV = 240 × 240 mm; matrix = 256 × 256; slice thickness/gap = 1.5mm/1mm • Used for anatomical alignment to MNI template, generation of tissue type probability masks and ROI selection • Image Preprocessing • ASL control and label images motion corrected to initial image and registered to 3DT1 using SPM99 • 3DT1 normalized to MNI template using SPM99 • All images up-or down-sampled to 2x2x2 mm resolution • 3DT1 images used to generate gray matter, white matter and CSF probability masks using SPM99 • Single Voxel/ROI Analysis • Whole brain voxelwise comparison were done using SPM99 fixed effects model corrected for multiple comparisons • 17 ROI’s identified from PickAtlas, both right and left and filtered by gray matter mask voxels with probability >0.8 • Cingulate Gyrus,Cuneus, Fusiform Gyrus, Inferior Frontal Gyrus, Inferior Parietal Lobule, Insula, Lingual Gyrus, Middle Frontal Gyrus, Parahippocampal Gyrus, Parietal Lobe, Posterior Cingulate, Precentral Gyrus, Precuneus, Pulvinar, Superior Occiptial Gyrus, Supramarginal Gyrus and Temporal Lobe • CBF for each ROI calculated as average over voxels in the ROI • Global gray matter estimate average from voxels with P>0.8 for gray matter in probability mask • Multivariate Analysis • PCA on zero-meaned scans from both subjects and controls • Derivation of discriminant pattern from first 4 principal components plus constant image • Outcome measure in linear regression is CDR rating: AD=1, controls=0 • Bootstrap resampling to estimate robustness of voxel weights in covariance pattern • Perform analysis executed on point estimate 500 times, sampling from each group with replacement, leaving the group assignment intact • Compute Z-statistic for each voxel as ratio of voxel weight in covariance pattern to voxel standard deviation over the bootstrap process • Voxels with |Z|>2 are taken as robust and displayed in SPM glass brain (p<???) Conclusion Careful spatial registration and normalization permits analysis of CASL perfusion MRI data with both multivariate and univariate statistical procedures, characterizing baseline CBF differences between AD and HC. We have identified an AD-related covariance pattern that appears to hold considerable promise in predicting conversion to AD. More standard univariate methods, both voxel-wise and ROI based, also are good predictors so further studies, particularly of mild cognitively impaired subjects, are needed to decide the optimum approach Regardless of the details of the analysis, the existence of a sensitive and specific MR based diagnostic procedure for AD, as suggested by our results, would be considerable. Since perfusion maps can be acquired at the same time with structural and other images, a general diagnostic examination for AD, able to also quantify atrophy and identify other possible causes of dementia, appears to be a realistic possibility. We are currently applying this analysis to subjects with MCI to determine whether this covariance pattern can be used to predict conversion to AD. References






