Download
1 / 23
300 likes | 670 Views
Radiofrequency Ablation of Lung Cancer. Andrew R. Forauer, MD FSIR Interventional Radiology Dartmouth-Hitchcock Medical Center. I have no financial disclosures. (but am willing to entertain offers…). Modern Cancer Therapy. Chemotherapy. Radiation Therapy. Surgery.

E N D
Radiofrequency Ablationof Lung Cancer Andrew R. Forauer, MD FSIR Interventional Radiology Dartmouth-Hitchcock Medical Center
I have no financial disclosures (but am willing to entertain offers…)
Modern Cancer Therapy Chemotherapy Radiation Therapy Surgery
Interventional Radiology is emerging as a fundamental discipline involved in cancer treatment • Percutaneous ablation • Embolization techniques • Intra-arterial drug delivery
Radiofrequency Ablation (RFA) • Thermal (heat) based tumor ablation system • Most common clinical applications: • Liver • Kidney • Bone, other soft tissue
Mechanism of action Thermal energy damage to cellular proteins, enzymes, & nucleic acids Creates a volume of tissue necrosis & coagulation
Patient selection • Early stage patients who are good surgical candidates proceed to surgical resection • What about those with multiple co-morbidities and/or poor lung function? • Up to 50% of their mortality will still be Ca-related
Tumor selection • Solitary lesions (usually) • 3 cm or less • Non-small cell histology • Location • Safe & reasonable percutaneous route • No extension to hilum/mediastinum • Not contiguous with major vessels or nerves
Radiation Therapy Surgery Ablation
RFA vs Surgical Resection Image-guided Ablation Surgical Resection Higher patient impact Pathology available for margins Nodal status determined • Well tolerated, no incision • Reliance on post-ablation imaging • No assessment of nodes
Sublobar resection, RFA, & cryoablation compared • Overall 3-year survival: • 87% (SLR), 87% (RFA), 77% (cryo) * • 3-year disease free survival: • 61% (SLR), 50% (RFA), 47% (cryo) * • * No significant difference between the 3 groups Zemlyak et al., J Am Coll Surg, 2010
RFA vs External Beam Radiation Image-guided Ablation Radiation Therapy Effects on adjacent lung tissue & dosage limitations Multiple visits Fewer complications • Local therapy with less “collateral damage” • Single session, but repeatable • Potential for procedural complications
Radiation therapy (conventional EB) Surgical resection (LR, sub LR, VATS) No difference in DFS Ablation ? OS at 5 years: 15-30% OS at 5 years: 40-55% SBRT: Better at local dz control; OS @ 5 yrs ~50%
RFA outcomes Overall survival data in RFA series tends to reflect a population with more co-morbidities, but Ca specific survival is encouraging 1. Lencioni R et al. Lancet-Oncol, 2008; 9:621-628 2. Zemlyak et al., J Am Coll Surg, 2010
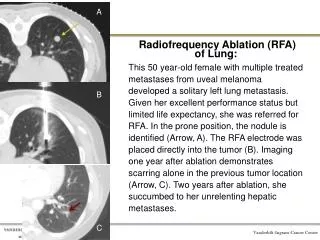
70 yr old patient w/ colorectal Ca & a LLL metastasis Peri-procedural CT during probe positioning Pre-ablation CT
Summary • RFA can be used to treat both primary & metastatic tumors • Doesn’t preclude other complimentary therapies • Patient selection is key/critical (not about the specialty, ego, or absolutes- its about thePATIENT)
Current areas under investigation in IR • Chemotherapy delivered via the pulmonary artery • Selective chemoembolization • Combining chemotherapy infusions with ablation procedures