Download
1 / 39
460 likes | 933 Views
Tryptophan Metabolism & its associated disorders. Dr. Ketki K Assistant Professor Dept of Biochemistry HIMS Varanasi. Content. Substances produced from Tryptophan Major Catabolic Pathway of Tryptophan Niacin Synthesis Synthesis & degradation of Serotonin

E N D
Tryptophan Metabolism & its associated disorders Dr. Ketki K Assistant Professor Dept of Biochemistry HIMS Varanasi
Content • Substances produced from Tryptophan • Major Catabolic Pathway of Tryptophan • Niacin Synthesis • Synthesis & degradation of Serotonin • Function of serotonin & effect of drug on Serotonin • Carcinoid tumor • Synthesis of Melatonin • Function of Melatonin • Hartnup’s disease
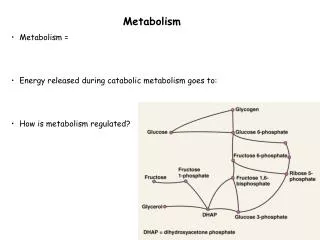
Tryptophan • Aromatic aa • Heterocyclic aa • Indole ring • Neutral • Essential • Polar • Both glucogenic & ketogenic
Major catabolic pathway of Tryptophan • Step1 : • Tryptophan pyrrolase or oxygenase cleaves the five-membered ring of the indole nucleus to produce N - formyl-kynurenine. • Tryptophan pyrrolase is Hemoprotein • The enzyme is inducible by corticosteroids.
Total 11 carbon atoms of tryptophan are catabolized as • Formyl group (1C which enters the one carbon pool), • Alanine (3C, entering the glucose pathway) • Acetoacetate (4C, going to ketogenic pathway). • Tryptophan is both glucogenic & ketogenic. • The remaining 3 carbons areremoved as 3 CO2 molecules.
Step 2: • Formamidasehydrolyses N-formyl-kynurenine, so Iiberates formate & kynurenine • Kynurenine formed in this reaction is a branch point with different fates
Step 3: • In the prominent pathway, kynurenine undergoes NADPH-dependent hydroxylation by kynurenine hydroxylase to give 3-OH-kynurenine • Kynurenine hydroxylase is inhibited by estrogen • Women are more susceptible to Pellagra
Step 4: • Kynureninase, a PLP - dependent enzyme acts on the 3-OH-kynurenine & splits off alanine (glucogenic pathway) & 3-hydroxy-anthranilic acid (which is used for NAD+ pathway) • Kynureninase is sensitive to vitamin B6 deficiency. • Due to the lack of PLP, kynureninase reaction is blocked & 3-OH-kynurenine/Kynurenine accumulates, which is diverted to form xanthurenic acid.
EIevated excretion of xanthurenic acid serves as an indication of B6 deficiency. • Administration of isoniazid, an antituberculosis drug-induces B6 deficiency & results in xanthurenic acid excretion in urine. • Defects in the activity of kynureninase (in B6 deficiency) cause reduced synthesis of NAD+ from tryptophan & manifestations of pellagra.
Step 5: 3-Hydroxyanthranilate is cleaved by an oxidase (Fe2+ dependent) to form an unstable intermediate, Aminocarboxy muconaldehyde • Step 6: Which undergoes decarboxylation to form amino muconate aldehyde • Step 7: Which undergoes deamination to form keto adipic acid • Step 8: Which undergoes decarboxylation to form Acetoacetyl CoA( Ketogenic)
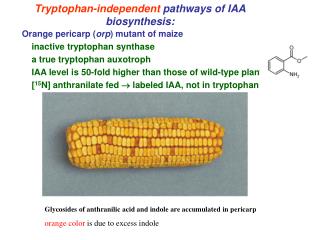
Conversion of tryptophan to indole acetate • Tryptophan undergoes transamination & deamination to produce indolepyruvate • Which is decarboxylated to indoleacetate • Which is excreted in urine.
Conversion of tryptophan to indole acetate Tryptophan Transdeamination NH3 Indole 3-pyruvate Decarboxylation CO2 Indole acetate Urine
Nicotinic acid Pathway of Tryptophan • 97% molecules of tryptophan: goes for major metabolic pathway, 3% : diverted at 3-OH-anthranilic acid to form NAD+ • QPRT : rate limiting enzyme • 3-OH-anthranilic acid to Quinolinic acid • Quinolinic acid undergo decarboxylation to form Niacin/nicotinic acid
Nicotinic acid to nicotinate mononucleotide(NMN) by the enzyme quinolinate phosphoribosyl transferase (QPRT) in presence of PRPP to PPi • From nicotinate mononucleotide to desamido NAD+ & NAD+ are synthesized.
60 mg Tryptophan = 1 mg Niacin • Maize eating population have tryptophan deficiency, leads to niacin deficiency & Pellegra like symptoms • Vitamin B6 deficiency leads to niacin deficiency
Serotonin pathway • Serotonin or 5-hydroxytryptamine (5HT) is a neurotransmitter, synthesized from tryptophan. • About 1% of the tryptophan is converted to serotonin. • The production of 5HT occurs in the target tissues.
Synthesis of serotonin • Site: Brain, mast cells, platelets, gastrointestinal tract mucosa & intestinal cells. • Step 1: • Tryptophan is first hydroxylated at 5th carbon by tryptophan hydroxylase to form 5-hydroxy tryptophan(5-HT) • It requires tetrahydrobiopterin as a cofactor.
Step 2: • 5-Hydroxytryptophan is decarboxylated by PLP-dependent decarboxylase to give 5-hydroxytryptamine (serotonin) • Platelets contain high concentration of 5HT.
Degradation of serotonin • Monoamine oxidase (MAO) degrades serotonin to 5-hydroxyindoleacetic acid (5-HIAA) which is excreted in urine. • Small portion of serotonin is conjugated with sulfate or with glucuronic acid & excreted through urine.
Functions of serotonin • Neurotransmitter, Involved in the regulation of cerebral activity (excitation) • Powerful vasoconstrictor & results in smooth muscle contraction in bronchioles & arterioles • Controls the behavioural patterns, sleep,mood,appetite, blood pressure & body temperature • Necessary for the motility of GIT • Platelets (platelet aggregation)
Its deficiency causes depression (That means ,it acts as an anti depressant) • Level decreased in depressive psychosis • Carbohydrate rich meal induce sleep,protein rich meal causes alertness, explain: • Protein rich meal→ traffic jam of aa in brain → tryptophan ,bulkiest amino acid , taken up very slowly • Carbohydrate rich meal → increased insulin release → decrease amino acid in blood → tryptophan easily enters in brain → it induces sleep
Carcinoidtumor/ Malignantcarcinoid syndrome • c/a Argentaffinomas (Tumor of argentaffin cells of gastrointestinal tract- mainly intestine & appendix) ↓ uncontrolled growth of these cells ↓ ↑ ↑ Serotonin ↓ C/F: Flushing,sweating,intermittent diarrhoea,fluctuating hypertension
In carcinoid syndrome, very high amount (up to 60%) of tryptophan is diverted for serotonin production ↓ impairs the synthesis of NAD+ ↓ Niacin deficiency ↓ C/F: Pellagra (dermatitis,diarrhoea,dementia,death)
Diagnosis • The excretion of 5-hydroxyindole acetatic acid in urine is tremendously elevated (upto 500 mg/day against normal <5 mg/day) in carcinoid tumor • The estimation of 5 HIAA in urine is used for the diagnosis of this disorder
Melatonin • Melatonin is a hormone. • Synthesized by the pineal gland. • Serotonin-produced from tryptophan-is acted upon by serotonin N-acetylase to give N-acetylserotonin. • Serotonin N-acetylase is a rate limiting enzyme.
N-acetylserotonin undergoes methylation, S-adenosylmethionine being the methyl group donor to produce melatonin • The synthesis & secretion of melatonin from pineal gland is controlled by light.
Functions of melatonin • Melatonin is involved in circadian rhythms or diurnal variations (24 hr cyclic process) of the body. • It plays a significant role in sleep & wake process. • Melatonin inhibits the production of melanocyte stimulating hormone (MSH) & adrenocorticotropic hormone (ACTH) • Melatonin also performs a neurotransmitter function
Hartnup’s disease • It is an hereditary disorder/Autosomal recessive • Cause: due to an impairment in the absorption and/or transport of tryptophan & other neutral amino acids from the intestine, renal tubules & probably brain. • Leads to deficiency of niacin & serotonin • Symptoms – pellagra like symptoms ,dermatitis, ataxia, mental retardation.
Diagnosis: 1) Low plasma levels of tryptophan & other neutral amino acids & their elevated urinary excretion (aminoaciduria) 2) Increased urinary output of indoleacetic acid & indolepyruvic acid: detected by Obermeyer test (Major excretory products of tryptophan comes in urine)
Treatment: • High protein diet with supplementation of niacin • Minimum exposure to sunlight
Question: • Explain why tryptophan deficiency leads to niacin deficiency? • Explain how carbohydrate rich meal induces sleep?/why do a person feels sleepy after eating heavy meal(rice)?