Download
1 / 20
270 likes | 873 Views
USANZ Perth 2010. Pathophysiology and Natural History of “BPH”. Henry Woo FRACS(Urol) Clinical Associate Professor University of Sydney. Pathophysiology of BPH. Precise molecular aetiology of the hyperplastic process is uncertain Observed increase in cell numbers

E N D
USANZ Perth 2010 Pathophysiology and Natural History of “BPH” Henry Woo FRACS(Urol) Clinical Associate Professor University of Sydney
Pathophysiology of BPH • Precise molecular aetiology of the hyperplastic process is uncertain • Observed increase in cell numbers • ?Epithelial and stromal proliferation • ?Impaired programmed cell death • Other influences • Androgens, oestrogens • Stromal-epithelial interactions • Growth factors • Neurotransmitters
Pathophysiology of BPH • Hormonal factors • Androgens essential for development of BPH • Testosterone is converted to dihydrotestosterone (DHT) in the prostate • Mediated by 5α reductase enzyme • DHT is the active androgen in prostate cell metabolism • Men do not develop BPH if • Castrated before puberty • 5α reductase deficiency • BPH partially regresses when • Surgical or biochemical castration • Pharmacological inhibition of 5α reductase
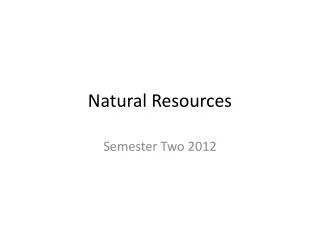
Even at low serum testosterone, conversion to DHT maintains intraprostatic androgen concentration The prostate concentrates androgen by converting testosterone to more potent DHT 30 25 20 15 10 5 0 DHT Prostate T or DHT concentrations (ng/g) Testosterone 0 100 200 300 400 500 Serum testosterone (ng/dl) Wright A, et al. 1999
Pathophysiology of BPH • Hormonal factors • Oestradiol and DHT act synergistically in producing BPH in canine prostates • Some correlation between serum oestrogens and BPH • Regulation of Apoptosis (Programmed cell death) • T and DHT suppress • Active cell death increased after castration
Pathophysiology of BPH • Stromal-Epithelial Cell interaction • Autocrine and paracrine signalling • Growth factors • Small peptide molecules that may • Stimulate • Inhibit • Cell division and differentiation processes
DHT and growth factors Stimulation of proliferation and survival Inhibition of proliferation and thestimulation of cell death BPH: imbalance of proliferative and apoptotic signals
Why Natural History Important? • Understand the progressive nature and complications of the disease • Understanding of risk factors for disease progression • Baseline variables • Dynamic variables • Understanding of where therapy can potentially alter the natural history of the condition
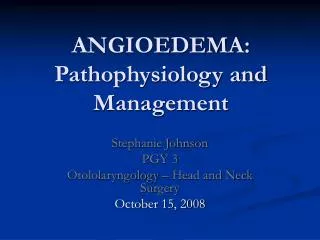
History and physical examination 100 Digital rectal examination 80 60 Prevalence (%) 40 20 0 40–49 50–59 60–69 70–79 Age (years) Prevalence of Clinical BPH Baltimore Longitudinal Study of Aging n=1,057; 30 years prospective study Arrighi HM et al. Urology 1991; 38 (Suppl): 4–8
Prevalence of Histological BPH Prevalence (%) 100 90 80 70 60 50 40 30 20 10 0 20–29 30–39 40–49 50–59 60–69 70–79 80–89 Pradhan 1975 Swyer 1944 Franks 1954 Moore 1943 Harbitz 1972 Holund 1980 Baron 1941 Fang-Liu 1991 Karube 1961 Roehrborn & McConnell, Campbell-Walsh Urology,9th Ed., Chapter 86 (2007)
BPH is a Progressive Condition PLESS = Proscar Long-Term Efficacy and Safety Study MTOPS = Medical Therapy of Prostatic Symptoms ALTESS=Alfuzosin 10 mg once daily long-term efficacy and safety study
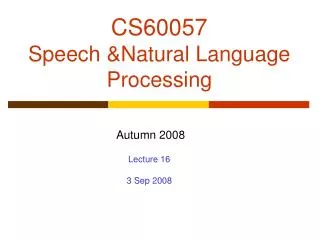
10 70–79 years 9 60–69 years 8 50–59 years 7 40–49 years 6 Cumulative incidence (%) 5 4 3 2 1 0 0 1 2 3 4 5 6 Time from baseline questionnaire (years) Cumulative incidence of AUR by follow-up Jacobsen SJ et al. J Urol 1997; 158: 481–487
PLESS – patterns of prostate growth (placebo-treated BPH) 20 Prostate volume (% change from baseline) 10 0 –10 Baseline* 1 2 3 4 Years *Mean prostate volume 55 mL Adapted from McConnell JD et al. N Engl J Med 1998; 338: 557–563
Impact of increased prostate volume • Men with large prostate glands compared with men with normal-sized or small prostate glands are: • 3.5 times more likely to have moderate or severe symptoms • 2.5 times more likely to have decreased flow rates • 3–4 times more likely to suffer AUR • 4 times more likely to need medical or surgical intervention Anderson JB et al. Eur Urol 2001; 39: 390–399
PSA is a strong predictor of an enlarged prostate and risk of BPH progression Increased PSA PSA predicts progression PSA predicts volume Greater risk of BPH progression Enlarged prostates Volume predicts progression
Cumulative incidence of BPH progression events MTOPS: Placebo-treated men Progression AUR BPH surgery Percent with event 25 20 15 10 5 0 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 Years from randomisation McConnell et al. NEJM 2003; 349: 2387–98
Olmsted County Study: baseline variables and risk of any treatment RR, 95% CI Qmax (mL/sec): >12* 12 1.0 2.8, 1.4–5.5 Prostate volume (mL): 30* >30 1.0 2.3, 1.1–4.7 Serum PSA (ng/mL): 1.4* >1.4 1.0 2.1, 1.1–4.2 *Reference category 0 0.5 1.0 5.0 10.0 15.0 Jacobsen SJ et al. J Urol 1999; 162: 1301–1306
Can We Predict BPH Likely to Progress? • Baseline variables • Dynamic variables
Baseline Variables on Progression • Baseline variables are important predictors of AUR and BPH related surgery • Age • Severity of LUTS (>12) • Flow rate (<12mL/s) • Increased PVR (>50cc) • Enlarged prostate (>30cc) • Increased PSA (>1.5ng/mL) • Data based upon Olmsted County Study and placebo limbs of MTOPS and ALTESS
Dynamic Variables on Progression • Worsening LUTS over 2 years increased risk of AUR or BPH surgery by 2-3X independent of baseline severity Meigs JB et al J Urol 1999; 162: 376–82 • Patients with stable PVR in MTOPS placebo group did not develop AUR McConnell JD et al. N Engl J Med 2003; 349: 2387-2398 • Failure to respond to alpha blockers was strong predictor of AUR and BPH surgery ALF ONE Study • Previous AUR episode, symptom worsening, lack of response to medical treatment and increase of the bother score are all significantly associated with occurrence of future AUR and/or BPH related surgery Emberton M et al. Urology 2005; 66: 316-322