Download
1 / 65
680 likes | 1.15k Views
Top Dermatological Tips on diagnosing skin lesions for busy GPs!. Louise Moss GP Moss Valley Medical Practice , Eckington 28 th March 2012. Aim for today. To feel more confident about how to diagnose and treat some common skin lesions within general practice. Remember,

E N D
Top Dermatological Tips on diagnosing skin lesions for busy GPs! Louise Moss GP Moss Valley Medical Practice, Eckington 28th March 2012
Aim for today To feel more confident about how to diagnose and treat some common skin lesions within general practice. Remember, common things occur commonly!
So what do we need to cover? • In 2009 I reviewed the sorts of skin conditions referred to my GPwSI clinic to see if this would help plan teaching for GPs, practice nurses & registrars. • 229 patients were seen from 3 neighbouring practices in a GPwSI community clinic
A rash lesion? 60% were lesions
80% of lesions referred include… • Possible Skin cancer • Benign naevi • Seborrhoeic warts • Actinic Keratosis • How can you increase your confidence?
The majority of these can be managed in primary care • Benign Naevi • Actinic keratosis • SeborrhoeicKeratoses • Also need to be able to identify common skin cancers
Top tips for lesion recognition • Take a good history- sun exposure, pmh/fh • Have a careful look with good light & magnification • Touch and feel- stretch the skin, if there’s a crust what’s beneath? • Look elsewhere for other examples • Is there a pattern?
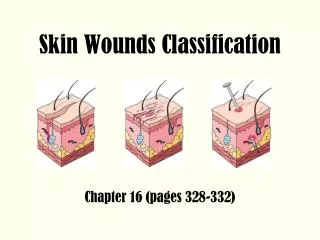
DESCRIBING SKIN LESIONS Site and size- record measurement Colour Surface or Texture Type of lesion Border/shape Attacehment to other structures Single or multiple/ arrangement of lesions IF YOU LOOK CAREFULLY YOU WILL BE ABLE TO DIAGNOSE WITH MORE CONFIDENCE!
Basal cell carcinoma What to look for.......... • Shine • Superficial telangectasia • Rolled edge • Spots of pigmentation • Ulceration • A history of slow growth & bleeding on sun-damaged skin
Don’t forget there are different types…… • Nodular/cystic • Superficial • Morpheic • Pigmented
Stretch the skin and look from the side............. YOU NEED TO TOUCH!
Squamous cell carcinoma • Rapidly growing • Tender • Indurated base • On sundamaged skin • ? Immunosupression • ? Worked in tropics
Solar (Actinic) Keratoses • Common sun exposed sites in older people UK >40yrs 15%men, 6%women • Forehead, face, back of hands, bald scalp of men, and ladies legs • Rough, raised and irregular, like stuck on cornflakes
Importance • Marker of sun damaged skin (so BCC/SCC/Melanoma risks all raised) • Malignant change MAY occur in AK • Quantitative evidence poor • Probably <1/1000 • Some remit spontaneously
Treating Actinic Keratoses in primary care • Why – very common • NICE IOG skin cancer 2006 : Patients with precancerous lesions may be treated entirely by their GP Exclusions: Diagnostic uncertainty Thick lesions Indurated or tender base – risk of scc Lesions in immunosupressed patient
AK- Treatment options • Do nothing- age/life expectancy/thin lesions • Single or multiple scattered AKs • Cryotherapy 5-10s FTC - • Curettage & cautery – useful if slight uncertainty/ensure base is included in histology specimen • Efudix – 5 flurouracil cream • Solareze – diclofenac 3% ( Bd for 3/12) • Excise if malignancy is suspected • Thick/tender/indurated/rapid growth • Multiple AKs/Field change – Efudix secondary care may use imiquimod ( Aldara) Can use Solareze – less irritant/ less effective Top up with Li N2 if needed for few residual lesion
How to use Efudix..... • Topical fluorouracil (5FU) is a topical cytostatic preparation that selectively destroys sun damaged skin cells with little injury to normal skin. • Useful for treating actinic keratoses that occur over a wide area and for Bowens Disease. • Not for very large or thick lesions with an infiltrated base:- refer these to exclude Squamous Cell Carcinoma.
Efudix treatment....... • Apply at night with a finger or cotton-bud..... • Avoid the eyes, lips and nasolabial folds. Don’t do too much at once! • Wash off the following morning.... • Apply daily for 2 weeks, unless the skin becomes tender and sore before then. If there is little or no change at 2 weeks then apply twice daily until ... • The skin becomes red, tender and a bit weepy. It may resemble a superficial burn. • This signals effective treatment and should take 10-28 days. Stop & allow to heal. Review after 1 month. • Early redness with mild stinging is not a sufficient end point!
Treating AK in primary Care • Look for other skin lesions • Advice re sun protection – 25% of lesions may regress • Inform patients that they may develop more lesions and which changes need to be reported Resources: Efudix leaflets PCDS.org.uk NED guideline
Solar (Actinic) Keratoses ALWAYS EXCISE (or refer) IF THICK, INDURATED OR TENDER LESIONS. • Be careful of causing a leg ulcer by excessive cryotherapy or Efudix on the lower leg • CUTANEOUS HORNS are better excised or curretted off with a good chunk of base
Cutaneous horn • Can arise from AK, keratoacanthoma,viral wart or SCC • Need excising to get histology • If no induration –could be curretted off with a good scoop of base for histology
Bowen’s disease • Full thickness dysplasia • 2-5% chance of developing SCC • Common lower legs/ hands/ face • Slow growing sharply demarcated scaly plaque