Download
1 / 53
530 likes | 770 Views
Competition and Monopoly. HSPM 712. Competition. How supply and demand work How “efficient” a market is As well as how equitable … depends on competition. Competition in insurance, for example. Textbook ideal: Lower price Better coverage -- Higher medical loss ratio

E N D
Competition and Monopoly HSPM 712
Competition • How supply and demand work • How “efficient” a market is • As well as how equitable • … depends on competition
Competition in insurance, for example • Textbook ideal: • Lower price • Better coverage -- Higher medical loss ratio • Oops! I mean “health benefit ratio.” • Better service • We get that (?), but also • Underwriting (higher premiums for the predictably sick) • Pre-existing condition exclusions • Retroactive cancellation
Textbook competition • Each firm is a price-taker • Each is too small to influence market • Demand curve is flat • Each firm expands production to the rate at which its marginal cost rises to equal the price. • The price sends a good signal to consumers. • What you pay equals the opportunity cost
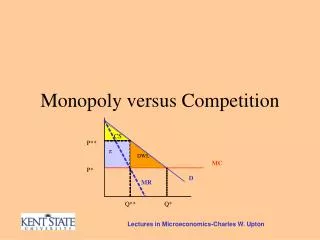
Textbook monopoly • Firm is price-maker • Demand curve has a slope • Seller restricts production • To raise the price • Leads to “welfare loss” or “consumer surplus” loss • Similar math to welfare loss from moral hazard in health insurance
Monopoly theory and antitrust laws • Monopoly and Competition Theory • "Monopoly" means one seller. It comes from Greek words meaning one (mono) seller (polein, which is Anglicized to "poly"). The term is used broadly to include industries of several sellers who act as one. The correct term for a "buyers' monopoly," where there is only one buyer, is "monopsony." • "Oligopoly" means a small number of sellers. The automobile industry is an example of an oligopoly. So is the hospital services industry in most small to medium-sized market areas.
Monopoly theory and antitrust laws • Monopoly and Competition Theory • Where is the dividing line between oligopoly and competition? The functional distinction is this: An oligopoly exists if one seller's actions can affect another seller's demand.
Structure, Conduct, and Performance • Economists analyze a market under three categories: Structure, Conduct, and Performance. • Structure is the context in which the actors in the market make their decisions. • Conduct is what decisions the actors make. • Performance is what we get as a result in terms of efficiency and equity.
Structure • Concentration: How many sellers are in the market and how big the bigger sellers are relative to the market as a whole. • Barriers to entry: How hard it is for a new firm to enter the market. Another way to think of this is: Are there potential competitors? • Product differentiation: Can you tell one firm's product from another's?
Conduct • Collusive behavior. Do the firms attempt to act as one? • Competitive behavior. Do the firms attempt to undercut each other? • Product differentiation. How do the firms try to distinguish their products?
Performance • Whether costs are minimized • Whether prices are high relative to cost • Quality • Pace of technological progress and innovation.
Structure-Conduct relation • Structure determines whether conduct matters. • Conduct doesn't matter in a perfectly competitive market, because any firm that doesn't minimize cost and keep its price low is out of business. • Conduct matters in monopolized markets. The monopolist may or may not take advantage of its position. • Conduct is most complex in oligopolized markets. An oligopoly can act like a monopoly, like competition, or like something else that conforms to neither of those models.
Natural monopolies • Natural monopolies -- if it is most efficient to have one seller serve an entire market. Local utility service may be an example, because it would be costly to have two sets of water pipes, electrical lines, or telephone lines to each house.
Natural oligopolies • Industries may be natural oligopolies, if there are economies of scale (larger size is less costly) to the point that the minimum efficient size firm is a substantial portion of the market. In automobiles, for example, minimum efficient sizes are large enough that it is doubtful that there could be more than a dozen or so mass-market automobile companies world-wide.
What monopolies do (that we don't like) • Restrict output and raise price • Transfer income to themselves, a distributional issue. • Efficiency is lost, because society forgoes the opportunity to turn relatively low value resources into relatively high value products. • Allow costs to rise, thanks to lack of competitive pressure. (Allocation issue.) • Retard or distort innovation, to defend the monopoly. (Allocation issue.) • Concentrate political power.
Antitrust laws Laws against monopolies in the United States: • Sherman Act of 1890 • Clayton and Federal Trade Commission Acts of 1914.
Sherman Act • The Sherman Act of 1890 makes it illegal to "monopolize, or attempt to monopolize, ... any ... trade or commerce..." • This law is aimed at market structure. The U.S. Justice Department has the responsibility for enforcing this law.
The Clayton and Federal Trade Commission Acts of 1914 • Prohibit monopolistic mergers and certain other forms of anti-competitive behavior. • These laws are aimed more at conduct. • The Federal Trade Commission was established by this legislation to enforce this law.
Justice Dept. and the FTC • That's why we have two government agencies, Justice and the Federal Trade Commissin, involved in antitrust law enforcement. • In the 1990’s, for example, it was the FTC that required Columbia/HCA to sell its Aiken hospital when it acquired a hospital in Augusta. • Also back then, the Justice Department sued two hospitals in Dubuque, Iowa, that were merging to form a local monopoly.
“Antitrust” • Calling anti-monopoly laws "antitrust" has its roots in the 1880's. • The "trust" was a specific form of corporate organization used by Standard Oil as it grew by merger towards being a national oil refining monopoly. Stockholders in corporations joining Standard Oil gave their shares of stock to Standard Oil. In return they got trust certificates giving them part ownership of Standard Oil. • State courts declared this arrangement illegal under then-existing state corporation law. • Standard Oil might have had to break up, but New Jersey came to its rescue by legalizing the holding company, allowing New Jersey corporations to own shares in other corporations. (Today, every state allows this.) • Standard Oil dumped the trust form of organization, moved its corporate headquarters to New Jersey, and became a holding company. • Nevertheless, the press applied the term "trust" to all large firms that were attempting to monopolize their markets, and the term has stuck to this day.
State antitrust exemptions relevant to health care • Federal McCarran-Ferguson act (1945) • Insurance is “commerce” and can be regulated by the U.S. and the states • The Sherman Act does not apply to insurance companies in states that regulate insurance. • This exemption of state-regulated industries from antitrust law is why Palmetto Health Alliance has a Certificate of Public Advantage.
Measuring structure The concentration ratio • is the portion of the market controlled by the top X number of firms. • You choose the X. • Pretty straightforward, if you have market share data.
Measuring structure • The Herfindahl-Hirschman Index (HHI) • The HHI measures concentration with the sum of the squares of the market shares of all the firms in the market. • An HHI near 0 indicates that no firms are large relative to the market -- a competitive structure. • An HHI of 1 means that there is just one firm in the market -- a monopoly structure.
Palmetto Health’s Certificate Of Public Advantage • Revenue per patient* will not rise faster than inflation • Will not monopolize medical practice • Savings given to community • Savings were anticipated from reduced duplication, spreading fixed cost over more patients • * adjusted for case mix
COPA irony • A COPA must be actively enforced by the state. • Otherwise, a Federal court might find that the COPA was not being strictly enough enforced to provide immunity from Federal antitrust action. • Hospitals "will be forced to monitor and even encourage active state participation as a security measure against antitrust liability." • Palmetto Health finances its own regulation, by giving DHEC money to pay for independent audits of PHA’s COPA compliance.
Diagnosis-Related Groups for Hospital Payment • Medicare introduced DRGs in 1983, phasing it in through 1988. SC Medicaid adopted DRG-based payment in 1986. Modified to hybrid system in 1987. • DRG-based prospective payment puts every patient into one of about 600 DRGs, according to the patient's diagnoses. • The DRG determines the payment to the hospital (except for very long stay outliers).
Diagnosis-Related Groups for Hospital Payment • Each DRG has a "weight" that represents the cost of treating such a patient relative to the average of all patients. • Payment = (The dollar amount for a DRG with weight = 1) multiplied by the weight of patient’s DRG. • Adjusting one dollar amount adjusts all the payments.
OBS DRG DIAG1 DIAG2 • 1 391 V3000 • 2 391 V3001 • 3 391 V310 • 4 391 V3000 605 • 5 391 V3000 7661 • 6 391 V3000 • 7 391 V3001 • 8 391 V3001 7661 • 9 391 V3000 605 • 10 391 V3000 • 11 391 V3001 • 21 391 V3000 • 22 391 V3000 • 23 391 V3000 7746 • 24 391 V3101 • 27 391 V3000 7746 • 28 391 V3000 7661
OBS DRG DIAG1 DIAG2 DIAG3 DIAG4 DIAG5 • 1 390 V3000 7525 • 2 390 7786 7660 • 3 390 V301 7526 V718 • 4 390 V3000 7526 • 5 390 V3101 7784 • 6 390 V3000 4279 • 7 390 V3000 37205 • 8 390 V3000 76408 • 9 390 V3000 7526 • 10 390 V3000 7706 • 11 390 V3001 71965 7706 7746 • 12 390 V3000 7661 74910 • 13 390 V3000 7793 • 14 390 V3000 7706 • 15 390 V3000 75501 • 16 390 V3001 7526 • 17 390 V3001 V718
OBS DRG DIAG1 DIAG2 DIAG3 DIAG4 DIAG5 • 1 389 V3000 7701 • 2 389 V3001 7731 • 3 389 7701 7718 V3001 0389 7792 • 4 389 7718 • 5 389 V3001 7708 5531 • 6 389 V3000 76408 7731 • 7 389 V3000 7661 7731 • 8 389 V3101 7731 • 9 389 V3000 7731 • 10 389 V3000 7731 • 11 389 V3000 7454 • 12 389 V3000 7708 • 13 389 V3001 7731 • 14 389 7756 7824 • 15 389 V3001 7708 7718 75462 7746 • 16 389 V3001 7795 7863 7706 • 17 389 7732 7526
Resource-Based Relative Value System for physician payment • In the late 1980s, Medicare led a direct attack on how physicians set their prices. Medicare implemented the Resource-Based Relative Value System for paying doctors. • It's now used, in various forms, by private as well as public payers.
RBRVS = DRGs for doctors? • No • DRG-based payment is prospective. It pays a certain amount per case, regardless of what resources the hospital puts in to the patient’s care. • RBRVS is fee-for-service payment
RBRVS = DRGs for doctors? • But Yes in the sense that • Both came from the US government • Both simplify payment-setting • Both based on giving a weight to each unit of service • Weight is proportional to the cost of the service • Costs are determined by formula, not existing market prices • Payment = (Payment for a service with weight = 1) × (Weight of the service)
Historical context • Roe, B.B., "The UCR Boondoggle: A Death Knell for Private Practice?" N Engl J Med, July 2, 1981, 305(1), pp. 41-45. • Medicare used Usual and Customary Rates as the basis for pricing doctor services. • Invited abuse. In 1981, a heart surgeon could do three 2-4 hour coronary bypass surgeries per week at $2500 each and make $350,000 annually.
RBRVS • RBRVS was intended to set fees by simulating the fees the market would have set if the market functioned properly. • With prices having a consistent relationship with cost. • Hsiao, W.C., Braun, P., Dunn, D., Becker, E.R., DeNicola, M., Ketcham, T.R., "Results and Policy Implications of the Resource-Based Relative-Value Study," N Engl J Med, September 29, 1988, 319(13), pp. 881-888. • This article, which is printed second in the original magazine, gives the general idea of RBRVS.
Physician work measure for RBRVS • Hsiao, W.C., Braun, P., Yntema, D., Becker, E.R., "Estimating Physicians' Work for a Resource-Based Relative Value Scale," N Engl J Med, September 29, 1988, 319(13), pp. 835-841. • This article (printed first in the NEJM issue) looks specifically at how they measured the physician's work entailed in any particular procedure.
The goal • Hsiao, an actuary by training, was later a major consultant to the Taiwan government for the reform of its health insurance system. • Here, he suspected that physician fees were out of proportion to cost, with some surgical specialties much more handsomely reimbursed than primary care. • Making the fees proportional to cost would encourage physicians to pursue careers in "primary care, rural practice, and out-of-hospital services," rather than flocking to surgical specialties.
RBRVS formula • RBRV = (TW)(1+RPC)(1+AST) • Resource-Based Relative Value = (Total Work)× (Specialty Practice Cost Index)×(Specialized Training Cost Index) • Specialty practice cost is hired labor and capital • Specialized training cost is the opportunity cost of spending time in residency.
Total Work formula • Total Work = Time×(Complexity Index) • Complexity index = “sweat factor” • Includes Pre- + Intra- + Post-service work • Based on surveys of physicians
Compares actual Medicare payments with what Medicare would pay if proportional to RBRV and total-payment-neutral