Download
1 / 60
600 likes | 789 Views
Gram negatives: Mechanisms of Resistance & Lab detection. Johann DD Pitout MD, FF Path (SA) University of Calgary Calgary Laboratory Services Calgary, Canada johann.pitout@cls.ab.ca. Transparency declaration. Research grants from Merck Frosst, Wyeth and Astra Zeneca

E N D
Gram negatives: Mechanisms of Resistance & Lab detection Johann DD Pitout MD, FF Path (SA) University of Calgary Calgary Laboratory Services Calgary, Canada johann.pitout@cls.ab.ca
Transparency declaration Research grants from Merck Frosst, Wyeth and Astra Zeneca Speaker for Merck Frosst 2 2
Overview Introduction Clones, stones and bones… Newer ß-lactamases Laboratory detection Emergence of clones in Enterobacteriaceae Summary 3 3
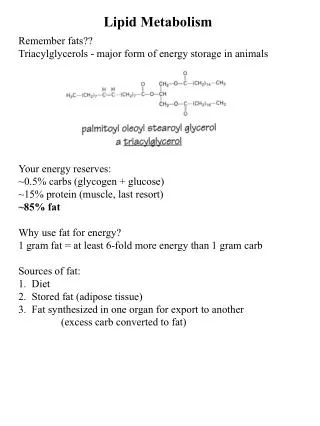
Why Enterobacteriaceae? • NB causes of serious bacterial infections: • Community • Hospital • Several species: • E. coli (ExPEC) • K. pneumoniae • Salmonella spp • Surveillance: • Top 5 community and hospital pathogens Am J Med 2006;119(sup1):S62-70
Why Resistance? • Resistance is concern: • 3rd GenCephs • Carbapenems • Fluoroquinolones • Empiric treatment • complicates antibiotic selection • Inadequate initial Rx (AAC 07;51:1987) • risk for mortality • health-care costs (AAC06;50:1257 Trends Microbiol 2006;14:413-20
What is a clone? • Definitions: • Isolate, strain, clone • Clone: • Isolates with identical phenotypic+genotypic characteristics • Different sources/time • Typing methods: • MLST • PFGE • PCR fingerprint (MLVA) CMI 2007;13:1-46
MLST • Sequence variation • Housekeeping genes • Evolutionary relationship • Comparing isolates • NOT outbreaks • ST’s and CC’s • E-BURST AnnRevMicro 2006;60:561-88
PFGE • Restriction of genomic DNA • Rare-cutting enzyme • +++ discrimination • Excellent outbreaks • Various species • But not portable: • Labour intensive • ? Reproducible • Time consuming CID 2007;44:418-23
Newer ß-lactamases 12 12
Clinical Case no 1 3 month girl with diarrhoea Watery with mucus Abnormal growth parameters Admitted and Rx Previous diarrhoea Other family members Older sister and Dad Salmonella enterica serotype Newport 13
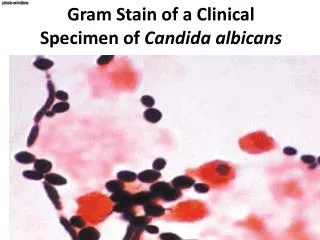
Salmonella spp. Susceptibility CFZ >64 TZP >64/4 CAZ 16 CRO 16 FOX >64 FEP <16 ATM 16 CIP <0.25 GEN <8 IPM <2 CLSI ESBL confirmation test: • CAZ 12mm • CAZ + CLAV 15mm • CTX 16mm • CTX + CLAV 16mm • Neg ESBL test 14
CTT CTT +PBA 15
AmpC ß-lactamases Chromosomal • Organisms: • Enterobacter, Serratia, Citrobacter, Pseudo. • cephalosporinases • inducible • not inhibited by c,t,s • eg.: AmpC Plasmid • Organisms: • Klebsiella, P. mirabilis, Salmonella spp. • cephalosporinases • constitutive/inducible • not inhibited by c,t,s • eg.: CMY, FOX, DHA, ACC ClinMicroRev 09;22:161-82 16
E. coli and AmpC’s mutations Plasmid-mediated AmpC Weak promoter Strong attenuator DMID 01;41:57-61 17 17
Plasmid-mediated AmpC’s R to cephamycins some cephalosporins, penicillins Not carbapenems Multiresistant Organisms: K. pneumoniae,E. coli, Salmonella spp Origin Extended-spectrum cephs ClinMicroRev 09;22:161-82 18 18
Laboratory detection No guidelines Not all cephamycin/3rd GC R = AmpC Phenotypic tests Inhibitor-based approaches Disks: boronic acid and others AmpC E-test: cloxacillin Multiplex PCR ERAIT 08;6:657-69 19
Clinical case no 2 47 yr F with recent travel ER with fever, dysuria, frequency Exam: T 39.2ºC supra-pubic and renal tenderness Diagnosis of UTI 2 sets of BC, urine Rx ciprofloxacin, referred to HPTP Next day blood cultures positive 22
Escherichia coli Susceptibility CFZ >64 TZP 64/4 CAZ 16 CRO >32 FOX <8 FEP 16 ATM 16 CIP >4 GEN >16 IPM <2 CLSI ESBL confirmation test: • CAZ 22mm • CAZ + CLAV 23mm • CTX 8mm • CTX + CLAV 20mm Pos ESBL test 23
Extended-spectrum ß-lactamases Early 1980’s World-wide Hydrolyse: cephalosporins, penicillins, monobact not: cephamycins, carbapenems Inhibitor sensitive clav, sulb, tazo Types Enterobacteriaceae Clinically relevant AmJMed 97;103:51-9 24
CLSI guidelines 2010 MIC ≥ 1 CTX/CRO ≥ 2 CAZ Zone ≤ 26mm CTX, ≤ 23mm CRO, ≤ 21mm CAZ No confirmatory test for therapy but useful for infection control/epidemiology
Detection of ESBLs • CLSI Screen positive • CRO: 1ug/ml and • CAZ: 1ug/ml • CLSI Screen positive • CRO: 1ug/ml and • CAZ: 1ug/ml Modified double disk FEP + CLAV • CLSI ESBL disk confirmation test: • CTX and CTX with Clav • CAZ and CAZ with Clav E. coli, Klebsiella spp, P.mirablis, Salmonella spp All other Enterobacteriaceace 26
Clinical case no 3 32yr M travelled in Southern India Admitted city Mysore: Hyperglycemia Developed upper UTI Rx with Ciprofloxacin Transferred to Alberta Upper UTI and prostatitis Rx with ERT
Escherichia coli (MH01) Suscept CFZ >64 TZP >64/4 CAZ >64 CRO >64 FOX >64 FEP >64 ATM >64 CIP >8 GEN >16 IPM 16 ESBL confirmation: • CAZ 6mm • CAZ + CLAV 6mm • CTX 6mm • CTX + CLAV 6mm AmpC boronic test: • CTT 6mm • CTT + PBA 6mm • ERT 6mm
Class B CHE’s Metallo-ß-lactamases (MBLs) Active site: Zn+ Inhibited by EDTA R to all ß-lactams except: monobactams Chromosomal (Steno) Types: IMP, VIM, SPM, GIM, SIM, AIM, KHM, DIM, NDM ClinMicroRev 2005;18:306-25
NDM ß-lactamases 1st report from Sweden (AAC 2009;53:5046-54) Worldwide Widespread in Subcontinent (Lancet ID 2010 10;597-602) India, Pakistan, Bangladesh Associated with travel (medical tourism) Organisms: E. coli (community) Klebsiella spp. (hospital) MultiR ? Fatal cases JAC 2011;66:689-92
Clinical case no 4 CAP external quality assurance program Klebsiella pneumoniae Urine; significant colony count Adult Diabetic patient Neurogenic bladder ICU for 2 weeks Recently hospitalised in New York 32
Klebsiella pneumoniae Susceptibility CFZ >64 TZP >64/4 CAZ >64 CRO >64 FOX >64 FEP 16 ATM >64 CIP >8 GEN >16 IPM 2 ESBL confirmation: • CAZ 10mm • CAZ + CLAV 13mm • CTX 11mm • CTX + CLAV 14mm AmpC boronic test: • CTT 10mm • CTT + PBA 22mm • ERT 6mm 33
Class A CHEs Different types (e.g.SME) KPC ß-lactamases K. pneumoniaeCarbapenemase 1st reported late 1990’s North Carolina Hydrolyze all ß-lactams Including carbapenems Inhibited by clavulanate Types: KPC 2-??? Klebsiella Producing Chaos Lancet Infect Dis 2009;9:228-36 35
CLSI June 2010Carbapenemases & Enterobacteriaceae MIC ≥ 0.25 ERT, ≥ 1 IPM/MER/DOR Zone ≤ 22 mm ERT/IPM/MER/DOR No confirmatory test for therapy if I or R to all carbapenems tested but OK for infection control/epidemiology
>0.25 ++false positives with ERT Use MER Multiplex PCR
CTX-M ß-lactamases Active CeftoTaXime 1stMunich activity CTX by tazobactam 40% similarity to SHV/TEM Originate fromKluyvera spp. Insertion element: ISEcp1 Divided into 5 groups Groups 1, 2, 8, 9, 25 Curr Opin Microbiol 2006;9:466-75 40 40
1989 1986 1990s 1989 CTX-M-type ESBLs: first reports Matsumoto et al. AAC 1988; 32:1243 Bauernfeind et al. Infection 1990; 18:294 Power et al. AAC 2002; 46:602 41
The CTX-M pandemic: since 2000 Lancet Infec Dis 08;8:159-66 42
The CTX-M-15 pandemic: since 2003 Lancet Infec Dis 08;8:159-66 43
Dissemination of CTX-M-15 MLST profile ST131 Broadly disseminated Homogenous virulence genotype IncF group plasmids 3 different profiles OXA-1, aac(6)-Ib-cr, TEM-1 JAC 08;61:273-81, EID 08;14:195-200 44
The clone ST131 pandemic: since 2006 IJAA 10; 35:316-21 45
MLST clone ST131(96/209 [46%]) 46 AAC 10;54:1327-30
E. coli from blood 47 47
Distribution of ST131 (69/134[51%]) AAC 09;53:2846-51 48
Characteristics of ST131 49 AAC 09;53:2846-51
What makes ST131 so special? ST131 CTX-M-15 • Uropathogenic • Phylo B2 • Certain VF’s • Adherence • IncF plasmids • R factors • Addiction systems IJAA 10;35:316-21 50