Download
1 / 58
580 likes | 873 Views
The Human Sexual Response. Amr Nadim, MD Professor of Obstetrics& Gynecology Ain shams Faculty of Medicine & The Women’s Hospital [Prof.amrnadim@gmail.com]. LEARNING OBJECTIVES. By the end of this lecture, you should be able to: Describe normal sexual response.

E N D
The Human Sexual Response Amr Nadim, MD Professor of Obstetrics& Gynecology Ain shams Faculty of Medicine & The Women’s Hospital [Prof.amrnadim@gmail.com]
LEARNING OBJECTIVES By the end of this lecture, you should be able to: • Describe normal sexual response. • List common sexual problems and their definition. • List causes and management of frigidity, dyspareunia, and vaginismus.
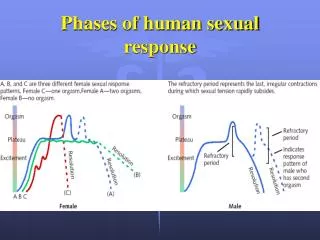
Human Sexual Response Masters and Johnson: four phases • Excitement/arousal • Plateau • Orgasm • Resolution 1956-1966
The sexual response cycle in humans progresses through four phases: • Excitement • Plateau • Orgasm (climax) • Resolution
Males: penile erection scrotal sac thickens, elevates Females: vaginal lubrication glans clitoris enlarges (similar to penile erection) nipples erect (myotonia: muscle contraction) breasts enlarge (vasocongestion inner lips of vulva swell and open, change in colour (darker) upper 2/3rds of vagina balloons cervix and uterus stand up: tenting effect angle of cervical opening more receptive to sperm Excitation: • Vasocongestion: pelvic area receives more blood in general, in particular to genitals. • Both Sexes: • sex flush (can happen later) • heart rate, respiration rate gradually increase • generalized myotonia
Plateau: • Both males and females continue vasocongestion to max • Heart rate, respiration rate and blood pressure continue to increase • Copious perspiration • Increased myotonia
Plateau (Cont’d) • Females: • orgasmic platform: outer third of vagina thickens, swells: condition sine qua non: without it, no orgasm • tenting complete • clitoris erect
Plateau (Cont’d) • Males: • Cowper’s glands secrete fluid through tip of penis. WARNING: may contain live sperm! • scrotum even higher and testicles bigger
Orgasm: • Males: Two stages: • contraction of seminal vesicles, vas and prostate • contraction of urethra and penis: ejaculation
Orgasm: • Females: • contractions of orgasmic platform • contractions of uterus • several orgasms possible if stimulation continues • oxytocin
Orgasm: • Both: • very high heart rate, blood pressure and breathing • intense myotonia
Health Benefits Associated With Orgasm • General Health • An orgasm at least once or twice per week appears to strength the immune system’s ability to resist flu and other viruses • Pain Relief • Some women find that an orgasm’s release of hormones and muscle contractions help relieve the pain of menstrual cramps and raise pain tolerance in general. • Better Sleep • The neurotransmitter dopamine, released during orgasm, triggers a stress-reducing, sleep-inducing response that may last up to two hours
Lower Cancer Rate • Men who have more than five ejaculations per week during their 20s have a significantly lower rate of prostate cancer later in life • Mood Enhancement • Orgasms increase estrogen and endorphins, which tend to improve mood and ward off depression in women • Greater Feelings of Intimacy • The hormone oxytocin, which may play a role in feelings of love and intimacy, increases fivefold at orgasm
Emotional Changes During Orgasm Based on EEG, MRI and PET scans done in the lab while subjects having an orgasm. • General emotional response: • coded in limbic association area, especially prefrontal cortex and cingulate gyrus. • Pleasure: • coded in basal forebrain, especially ventral tegmental area and its dopaminergic stimulation of the reward centres of the septal nuclei and the nucleus accumbens. • Euphoria: • probably by assymetric cortical activation • The proportion and intensity of each varies with each orgasm.
Resolution • Return to normal, muscles relax, breathing etc. back to normal, blood back to circulation from genitals. • Males • refractory period EACH PHASE MUST BE FULLY COMPLETED IN ORDER TO REACH THE NEXT ONE
SOME GENDER DIFFERENCES • Excitation: • women slower: • cultural expectations, socialization • pregnancy • It is very important for male partner to make sure she is ready for plateau stage
Plateau: • without orgasmic platform women can’t have orgasm. • Orgasm: • multiples for many women. Some women cannot go through resolution without several orgasms, vasocongestion persists. • Resolution: • women have no refractory period
“Pleasure centers”: (for arousal and orgasm) • Both: • genital area • Women (and some men): • nipples, breasts, G-spot • Men: • prostate • Many body areas can be: • ears, back of knees, neck, feet, abdomen, thighs, inside of elbows, scalp
Retrograde Ejaculation: • Two separate valves or sphincters, one to let urine into urethra, and another to let semen into urethra. When one is open, the other closes. In some cases, the semen valve is closed and the urinary valve that opens to the bladder is open. Semen flows into bladder. No ill effects.
Resolution: • Men: • longer refractory periods, 24 hrs. midlife, longer in old age. • Women: • no refractory periods ever.
Each phase shows age changes • Excitation: • Men: • fastest 16-20 years, then show decline • Middle Age: • very noticeable, need direct stimulation • Old Age: • need lots of direct stimulation • Women: • slower in teens, early 20s • faster 30’s on • Plateau: • Men: • capacity for longer with age • Women: • same, but never a big problem
Orgasmic: • Men: • intensity lessens from mid- to late 20s • Middle Age: • really noticeable • ejaculate less volume, less forceful • Resolution: • Refractory period increases
20 30 40 50 60 70 80 Females Intensity of Response Males Age
PHYSIOLOGY OF THE SEXUAL RESPONSE • Cognitive models: • Kaplan’s triphasic model: • sexual desire • vasocongestion • muscular contraction • Walen and Roth’s model: • emphasis on perception and evaluation, 8 steps, necessary for the arousal cycle to be completed
PHYSIOLOGY OF THE SEXUAL RESPONSE • Neural and hormonal involvement in sexual responses: • Parasympathetic: • arousal • Sympathetic: • orgasm • Spinal reflexes: • erection and ejaculation • Erection: • sacral cord responds to stimulation, sends message via parasympathetic to relax penile arteries: more blood flows to penis. Also, message to brain, awareness (not if spine severed above sacrum) • Ejaculation: • higher in spinal cord, message to sympathetic that causes muscle contractions. Also, message to brain, awareness, possibility of control
Women’s Neural Mechanisms: • Not yet well known • Controversy surrounding G-spot and female ejaculation. • One recent study found that sexual sensations can be transmitted to the brain via the vagus nerve, which is normally used for digestive processes.
PHYSIOLOGY OF THE SEXUAL RESPONSE • Higher Centres: • limbic system: septal region of the amygdala
PHYSIOLOGY OF THE SEXUAL RESPONSE • Experiments using electrical stimulation: • Erection centers found in the limbic system, both in monkeys and humans.
Hormonal Influences on Sex • Most Studied Sex Hormone: • Testosterone • produced by testes, ovaries and adrenal glands • important for sexual desire in both sexes
Hormonal Influences on Sex • Women have 1/10th the amount but are ten times more sensitive to it. • More testosterone in a normal person will not increase desire or response. • Most testosterone is ‘bound’, not available in this regard, ‘free’ testosterone is 2-5%. • Oxytocin, produced by the pituitary, important for female orgasm.
Chemistry of Attraction • DHEA (dehydroepiandrosterone): • secreted by adrenal glands, weak androgen. Most sex hormones and pheromones derived from it. • Same amount for males and females in bloodstream. • Pheromones: sexual signals for both sexes. • Oxytocin: released by the pituitary when touching or being touched by loved ones.
Chemistry of Attraction • PEA (phenylethylamine): called “the molecule of love”, produce euphoria, amphetamine-like substance produced in brain capillaries and in catecholaminergic terminals. • Low PEA levels associated with depression (some depressions successfully treated with PEA). • Some people become addicted to the PEA “high” and change partners frequently to get it, itis more abundant early in a relationship.
Chemistry of Attraction • Estrogen: makes women sexually attractive and receptive. Skin, lips, hair, fatty padding (curves), breasts, hips. • Testosterone: increases sex drive in both sexes, too much is counterproductive. • Endorphins: produced in the brain, released in response to touch and sex, produce positive feelings. • Progesterone: testosterone antagonist, lowers sex drive (in the pill as well), mild sedative, calming effect.
Chemistry of Attraction • Serotonin: neurotransmitter. At low levels intensifies sex drive, at high levels decreases it. Antidepressants elevate serotonin, decrease sex drive. • Dopamine: neurotransmitter associated with all pleasures, increases sex drive, promotes action. • Prolactin: decreases sex drive, especially in men.
Chemistry of Attraction • Vasopressin: • hormone produced by the pituitary, antidiuretic (water retention), increases blood volume and blood pressure, identified as the “monogamy molecule”, modulates testosterone, levels extremes of feelings, increases focus in lovemaking. • All these substances fluctuate in a 24 hr. cycle, also with age and environmental events. • The “high” of early love is short-lived (6-30 months). Cultural belief in passionate love forever not realistic.
PHYSIOLOGY OF THE SEXUAL RESPONSE • Hormonal Influences on Sex (Cont’d): • Hormones are NOT directly responsible for human sexual behaviour, as they are in most animals. • Psycho-social context and culture are the most important determinants. • In real life, people in good relationships say that sex is better than in casual situations.
PHYSIOLOGY OF THE SEXUAL RESPONSE • Anatomy and physiology of sex only give us an idea of how our biological equipment tends to work, but it does not give us an understanding of human sexual behaviour. Knowing car mechanics does not make you a good driver! • In order to get this, we need to explore our psychology, our communication styles, our culture/s, our interpersonal skills, etc.
Types of Sexual Dysfunction • Commonly the cause of sexual dysfunction is multifactorial and result in more than one dysfunction. • Primary sexual dysfunction: Those who never had normal sexual activity. • Secondary sexual dysfunction: Those who developed sexual dysfunction after a period of normal sexual activity.
Prevalenceof Sexual Complaints in Women 43% of women experienced a sexual problem 32% 28% 27% Percentage of Women* 21% *Women aged 18-59 years Laumann EO, et al. JAMA. 1999;281:537-544.
Comorbidity of Anxiety and Depression With Sexual Problems Increased association between anxiety or depression with sexual problems Odds Ratio* *Odds ratio for association between anxiety and depression and sexual problems Dunn KM, et al. J Epidemiol Community Health. 1999;53:144-148.
Comorbidity of Marital Difficulties and Sexual Problems Increased association of marital problems with arousal, orgasm, or enjoyment problems Odds Ratio* *Odds ratio for association between marital difficulty and sexual problems Dunn KM, et al. J Epidemiol Community Health. 1999;53:144-148.
Categories of Female Sexual Dysfunction Sexual desire disorders Hypoactive sexual desire disorder Sexual aversion disorder Sexual arousal disorder Female sexual arousal disorder Sexual orgasmic disorder Female sexual orgasm disorder Dyspareunia Vaginismus Noncoital sexual pain disorder Sexual pain disorders Basson R, et al. J Urol. 2000;163:888-893.
Physiological • Neurological problems • Cardiovascular disease • Cancer • Urogenital disorders • Medications • Fatigue • Hormonal loss or • abnormality • Psychological • Depression/anxiety • Prior sexual or physical abuse • Stress • Alcohol/substance abuse Female Sexual Dysfunction • Interpersonal • relationships • Partner performance and technique • Lack of partner • Relationship quality and conflict • Lack of privacy • Sociocultural • influences • Inadequate education • Conflict with religious, personal, or family values • Societal taboos
Sexual Desire Disorders • Hypoactive sexual desire disorder • Absence of sexual fantasies, thoughts, and/or desire for, or receptivity to, sexual activity, which causes personal distress • Sexual aversion disorder • Phobic aversion to and avoidance of sexual contact with a sexual partner, which causes personal distress Basson R, et al. J Urol. 2000;163:888-893.