Download
1 / 21
210 likes | 232 Views
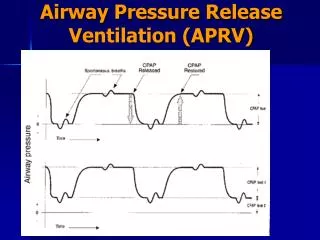
Explore the evidence, limitations, and conclusions of APRV usage in ARDS patients to optimize ventilator strategies and enhance recovery outcomes for critically ill individuals with acute respiratory distress syndrome.

E N D
Con Position: APRV should be used in ARDS Timothy Scialla, MD Assistant Professor Division of Pulmonary and Critical Care Duke University 09/07/2017
COI disclosure slide • I am a co-investigator for on-site clinical research trials sponsored by: • GSK • AstraZeneca • Sanofi • Genentech • NHLBI
ARDS epidemiology • 190,000 cases / year in the USA • 50% Moderate (PaO2/FiO2 100-200) • 25% Severe (PaO2/FiO2 < 100) • Mortality 40% • Early (underlying cause) • Late (sepsis / nosocomial pneumonia /MODS) • Ventilatory failure (ie. Hypoxemia) uncommon • High Morbidity (cognitive, psychological, physical)
The ARDS Industrial Complex • Nearly 2 decades of well-funded research • Multiple large randomized trials • Pharmacotherapy • Ventilator strategies • Hemodynamic monitoring/management • Lessons learned • Heterogeneous disease process • Different ARDS phenotypes • Few successes Extensive Animal Studies
Studies with mortality benefit • ARMA trial • Neuromuscular blockade in ARDS • Prone positioning in ARDS • All three: • Avoid ventilator-induced lung injury
The ventilator is an agent of harm Risk of overdistension injury 12 12 Lung volume 6 6 6 6 Risk of atelectasis injury Time
Lung Protective Strategies • “Low VT” strategy • Minimize stress and strain • Limit VT and plateau pressure (<30cm H20) • “Open Lung” strategy: • recruiting nonaerated lung regions • Keep open with adequate levels of PEEP. • Minimize hyperinflation and atelectrauma with alveolar recruitment.
ARDS Network Low vs. Traditional VT P=0.007 6 ml/kg 12 ml/kg • Absolute risk reduction = 9% (31% vs 40% mort) • Relative risk reduction = 22% Lower oxygenation Worse ventilation ARDS Network NEJM 2000
Lung Protective Ventilation and Knowledge Translation Needham et al. BMJ. 2012 • 180/485 patients (37%) never had LPV • 417/485 (86%) adherent 50% or less
NMB in early ARDS. Papazian et. al. NEJM. 2010 • 340 patients randomized • Sedative: Ramsey Level = 6 (very very sedated) • Cisatracurium group: • 15mg bolus followed by continuous infusion for 48hrs • Open label 20mg IV bolus of cisatracurium allowed in either group if Pplat>32. Adjusted Cox regression model: HR 0.68 (95% CI, 0.48 to 0.98; p=.04) Adjustments made for PaO2/FiO2; Pplat, SAPS II
Open Lung Strategy:Metaanalysis: High vs Low PEEP. • Higher PEEP (n=1136) Low PEEP (n=1163) • Higher PEEP: better PaO2 transiently (same at day 7) • Higher PEEP: Pplat; PEEP Briel et al. JAMA. 2010
Why these results? Responders Nonresponders Grasso et al. High vs Low PEEP. AJRCCM. 2005.
HFO: The perfect scenario Risk of overdistension injury Lung volume Risk of atelectasis injury Time
Avoid this Risk of overdistension injury Lung volume Risk of atelectasis injury Time
HFOV: Our curiosity with this mode has come to an end • OSCILLATE trial • 548 patients • HFO group • Increased sedation/paralytics • More pressors/high mean airway pressures • Less refractory hypoxemia • Increased mortality? N=146 P=.08 Ferguson et al. NEJM. 2013
Prone Positioning in ARDS: Mount Everest in Kansas • Recruited more severely hypoxemic patients • Prone group with higher PaO2:FiO2 ratio at days 3 and 5 • Prone group had lower Pplatrs lower at days 3 and 5 • NNT to prevent one death was 6 Guerin et al. NEJM. 2013
Pleural pressure in dependent and non-dependent regions Fessler and Talmor. Respiratory Care. 2010
APRV: Evidence & Limitations • Evidence • Limited, small, mostly trauma patients • One RCT: APRV vs LOVT • Intubated trauma patients at risk for ARDS • LOVT = SIMV (VT = 6ml/kg PS=10 cm H20) • Limitations • At Phigh: spont breaths can add to strech • Plow to Phigh: shearing/atelectrauma N=31 N=32 Maxwell et al. J Trauma. 2010
Conclusions • 2 decades of extensive prospective studies • APRV = 1 very small RCT (negative study) • Longer time on ventilator • No improvements in oxygenation • Trend towards more sedation! • Low tidal volume ventilation is GOLD STANDARD • Severe cases • Neuromuscular blockage • Prone ventilation • Neither requires tertiary care center/ high technology