Download
1 / 18
190 likes | 329 Views
ICU Discharges. SICSAG September 2009 Dr Richard A Burnett Intensive Care Medicine. INTRODUCTION. Pressure for Critical Care beds has increased Review of services More ICU beds More HDU beds Outreach teams MET teams Altered threshold for admissions. Overview.

E N D
ICU Discharges SICSAG September 2009 Dr Richard A Burnett Intensive Care Medicine
INTRODUCTION • Pressure for Critical Care beds has increased • Review of services • More ICU beds • More HDU beds • Outreach teams • MET teams • Altered threshold for admissions
Overview • Associated with increased mortality • ‘Critical to Success – The place of efficient and effective critical care services within the acute hospital’ (Audit Commission 1999) • Recommendations • Regular outcome audit of patients prematurely discharged or transferred to another ICU • Transfer arrangements be put in place with neighboring hospitals
Overview • ‘Comprehensive Critical Care – A review of adult critical care services’ (DoH 2000) • Re-emphasised the monitoring of case-mix adjusted mortality • Bed manager should ensure discharge from critical care takes place at an appropriate time of day • Long distance transfers/transfers outwith the agreed group of hospitals be recorded as an adverse incident
Overview • Quality Critical Care – Beyond ‘Comprehensive Critical Care’ • Reinforced and updated the recommendations of Comprehensive Critical Care • NICE • Acutely Ill Patients in Hospital – Recognition of and response to acute illness in adults in hospital • Transfer of patients from critical care to the ward out of hours (2200-0700) to be avoided • AND reported as an adverse incident
Outcome Measures • Policy documents highlight 6 potential outcome-based quality indicators • 3 on external transfers (to another unit) • All • Non-clinical • Outside the ‘transfer group’ • 3 on internal timeliness of internal discharge • Premature • Delayed • Out of hours
Consequences of OOH Discharges – ICNARC 2000 • Out of hours = variable descriptions • 22:00 – 06:59 • 20:00 – 07:59 • 2.7% in late 80’s vs 6% in mid-90’s
Objectives • To access the Ward Watcher data for the period 2000-2008 with reference to : • Highlighting the number of live discharges from ICU • Highlighting the reason for discharge • Out of hours and delayed discharges • (Re-)Establishing variables associated with increased mortality
Methods • Clinicians and epidemiologist • National Project Manager and National Clinical Coordinator • Systems analysts/statisticians • SICSAG executive for approval
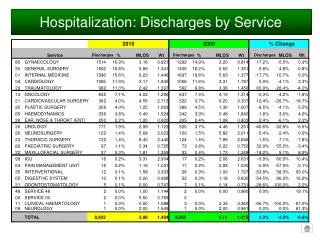
Methods • Looked at data between 2000-2008 • All live discharges from ICU’s in Scotland • 60,000 patients • Data extracted for : • time of discharge • reason discharged • delayed discharges • length of delay • discharge destination
Methods • Logistic regression model designed to assess associated risk of mortality for : • Out of hours vs In hours • Delayed discharge • Age • Gender • APACHE II • Operative vs Non-operative • Destination • More than one CHP
Odds ratios and corresponding 95% confidence intervals * p < .05; ** p < .01; *** p < .001
Discussion • Data set is robust when compared to the literature • Out of hours discharges have increased since 2000 • OOH discharges are consistently associated with poor outcome • Delayed discharges have more than doubled since 2000 • Delayed discharges stay on ICU an average of 0.75 days (currently) • The number of early discharges has fallen and the number discharged fully ready for non-icu care has increased