Download
1 / 39
430 likes | 641 Views
Exercise and Aging Skeletal Muscle. Brooks - Ch 32 Brooks - Ch 19 (p444-451). Outline. Aging introduction Physiological capacity and aging CV and skeletal muscle only Aging process Exercise Prescription. Aging. Decline of physiological capacity is an inevitable consequence of aging

E N D
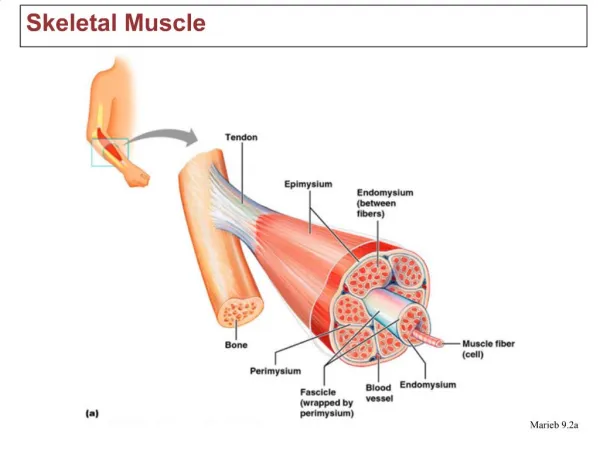
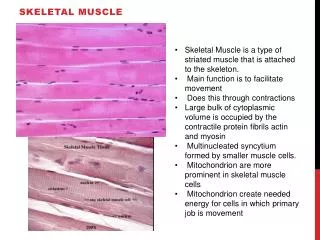
Exercise and Aging Skeletal Muscle • Brooks - Ch 32 • Brooks - Ch 19 (p444-451)
Outline • Aging introduction • Physiological capacity and aging • CV and skeletal muscle only • Aging process • Exercise Prescription
Aging • Decline of physiological capacity is an inevitable consequence of aging • physical inactivity may contribute to these declines • complicating the quantification of the effects of aging • Aging involves diminished capacity to regulate internal environment • Body structures are less capable and less resilient • Reduced capacity is evident in; • Reaction time, disease resistance, work capacity, and recovery time • Body composition with aging • inc % body fat / dec lean body mass • muscle size peaks at 25-30 yrs • Resting Metabolic Rate (RMR) • decline associated with decreased muscle mass
Life expectancy, Life span, and Morbidity • Lifestyle (diet, exercise) will influence performance and health with aging, but will not halt the aging process. • Life expectancy has changed dramatically in this century • 1900: 47 years ; 2000: 76 years • Maximum lifespan (100 years) has not changed • Quality of life, wellness, is important • North Americans only have healthy quality life during 85% of their lifespan, on average • Good lifestyle choices can compress morbidity - state in which they can no care for themselves • Reducing morbidity from 5-10 years to 1 or 2 can add quality years to your life
Physiological Capacity • Physiological functioning peaks ~ age 30 • Table 32-3 • ~.75 to 1 % decline per year after 30 • Declines in VO2 max, Q max, strength ,power, and neural function; also increases in body fat • All of theses factors can be positively impacted by training
Physiological Capacity • Maximal O2 consumption and age • VO2 max declines ~30% (age 20-65) • Fig 32-2 - (training and age vs VO2 max) • Significant individual variability • Similar declines with age in trained and untrained - trained has higher capacity • Due to decrease in max HR, SV, Power, fat free mass and A-V O2 difference
Physiological Capacity • Heart Rate and age • Sub max - HR lower at relative intensity but the same at any given absolute intensity • Cardiovascular drift is higher with age • Longer recovery time back to resting values from submaximal and maximal exercise • Increased cardiovascular drift • Decreased b- adrenergic responsiveness • decreased max HR • decreased contractility
Stroke Volume and Cardiac Output (Q) • Aging the hearts capacity to pump blood • Q and SV are less during exercise • Both relative and absolute intensity • Gradual loss of contractile strength due to • Ca ATPase and myosin ATPase activities and myocardial ischemia • Often, heart wall stiffens, delaying ventricular filling - dec SV… dec Q • The elasticity of blood vessels and the heart due to connective tissue changes. • Heart mass usually and there are fibrotic changes in the heart valves • Slower relaxation of ventricular wall • SV changes rely more on Frank Starling due to reduced contractility
Vascular System • Poor peripheral vascular tone • Varicose veins • Reduces venous return affecting EDV and SV • Vascular stiffness the peripheral resistance, the afterload of the heart. • peripheral resistance also raises SBP during rest and exercise (no change in DBP). • Capacity of autonomic reflexes that control blood flow is reduced • At rest circulation to periphery is poor (cold) • During exercise circ to periphery is too high • Greater incidence of orthostatic intolerance • Decreased plasma, red cell and total blood volume
A-V O2 difference • Dec with age - contributing to dec aerobic capacity • Decreases from 16 vol % (20 yrs) to 12 vol % (65 yrs) ( mlO2/dl) • Reductions due to • capillary/fiber ratio • total hemoglobin • respiratory capacity of muscle • in muscle mito mass • oxidative enzymes • However, A-VO2 is higher at any absolute exercise intensity with age
Skeletal Muscle • Loss of muscle mass and strength can severely impact quality of life • Muscle strength decreases approximately 8% per decade after the age of 45. • Aging results in a in isometric and dynamic strength and speed of movement. • Strength losses are due to: • size and # of muscle fibers and motor units • in connective tissue and fat • Severe loss of contractile elements - sarcopenia
Muscle Fiber Types • With age there is a selective loss of type II fibers, • is more rapid in the lower body. • available strength and power. • Muscle is less excitable, greater refractory period • maximum contractile velocity • There is loss of biochemical capacity with age. • [ ] of ATP and CP • in glycolytic enzymes (LDH). • There are no changes or slight in oxidative enzymes • *Controversy over whether there is a decrease in oxidative capacity or not with ageing • Some studies show higher AMPkinase activity at rest and after exercise - may have impact on type II fiber hypertrophy/atrophy • Aged muscle may have better metabolic economy and be more fatigue resistant
Gordon,SE et al Exerc Sport Sci Rev Vol 36 no 4 pp179-186, 2008
The Aging Process • Genetics has an important influence on length of life; genetics in concert with environmental factors affects the quality of that life • Aging may be related to; • accumulated injury, wear and tear, autoimmune reaction, problems with cell division, • abnormalities of genetic function • free radicals (ROS), radiation, toxins • Correlation between age and accumulation of oxidative damage due to ROS - Free Radical Theory of Aging • ROS act on lipids, protein and DNA • Causal role for oxidative stress in aging process now well supported • Eg Hydroxyl radical (OH˙) causes DNA lesions • Eg Superoxide anion thought to act on Mitochondrial DNA • oxo8dG - guanine oxidation often studied as it pairs with Adenine instead of Cytosine and a potential mutation
Portrait of typical 45 year old male and female, 1981 and 2007 Canadian Health Measures - Jan 2010, Statistics Canada
Aging, Lifestyle and Disease • Lifestyle choices (deconditioning) • Some people physically deteriorate with age due to a lack of exercise, obesity, poor diet, smoking, and stress. • Others are active and still fit in their 50s, 60s and 70s. • Disease and physiological function • Disease further complicates our understanding of the aging process- osteoarthritis, atherosclerosis • Sedentary death syndrome (SeDS) • Clear that adaptation to exercise has a genetic basis (plasticity) • Effort to find molecular proof that physical inactivity is an actual cause of chronic disease • Some researches want to move away from using sedentary individuals as controls in experiments - eg GLUT 4 • Sedentary Physiology • independent risk factor for CVD, some Cancers
Prolonged uninterrupted sitting, independent of physical activity may be a risk factor for chronic disease. Fig. 1. The movement continuum, illustrating the different focus of sedentary physiology and exercise physiology. METs, metabolic equivalent tasks.
Fig. 3. Illustration of accelerometer data portraying an active couch potato (moderate to vigorous intensity physical activity meeting guidelines considered ‘‘physically active’’ but also a high level of sedentary behaviour) versus an active non-couch potato (similar level of moderate to vigorous intensity physical activity but low level of sedentary behaviour). (From Dunstan et al. 2010a, reproduced with permission of Touch Briefings, European Endocrinology, Vol. 6, p. 21, # 2010.)
Fig. 4. Portrayal of significantly different patterns of breaks in sedentary time, based on accelerometer data from 2 different individuals (a ‘‘prolonger’’ and a ‘‘breaker’’). (From Dunstan et al. 2010a, reproduced with permission of Touch Briefings, European Endocrinology, Vol. 6, p. 21, # 2010.)
Dietary Restriction and Aging • Dietary restriction extends lifespan in rats and monkeys by 30-50 % • reduces age related diseases • Humans? - Okinawa diet 20% less calories, 300% vegetable intake, low in fat and sugar - results? • May retard basic metabolism and biological processes of aging • May suppress age-related pathologies - • found to impact immune system, protein turnover, bone loss, neural degeneration • Reduces oxidative stress by ROS through increased antioxidant activity • Observe significant decreases in oxo8dG DNA lesions in rodents
Resistance Training Response • Exercise training provides psychological benefits • Improved cognitive function, self efficacy and reduced depression • Training does not retard the aging process, it just allows the person to perform at a higher level - Fig 32.2 • Strength training • Relative strength with training are similar in young and old individuals. - Only short term studies available • Helps prevent loss of muscle mass and strength • Prevents bone mineral loss • Improves postural stability, reduces risks of falls and fractures • Mobility exercises improve flexibility and joint health
Endurance Training • Aerobic Endurance Training helps • Maintain CV function and enhances exercise capacity • Reduces risks for HD, diabetes, insulin resistance and some cancers • May attenuate age related increase in ROS DNA lesions (oxo8dG) • Similar improvements in Aerobic capacity for young and old • 6 months ~20% increase in VO2max • Observe • Dec submax HR at absolute load • Dec resting and submax SBP • Faster recovery of HR • Improvements in ECG abnormalities • Inc SV and Q • Elderly require a VO2max of ~20 ml/Kg to be independent • A conservative well structured program can bring most elderly to this level of fitness within ~3 months
Exercise Prescription • The principles of exercise prescription are the same • however caution must be taken with the elderly to the risk of injury. • Elderly have more abnormal ECG’s during exercise. • Start slowly with walking or swimming - low impact • Running, racket-ball… only when fit • Problems with using estimates of Max HR for prescribing intensity - considerably variation in the elderly • (Max HR range : 105 - 200 for 60yr olds) • Principles • Progress carefully with intensity and duration • Warm up slowly and carefully • Cool down slowly - to less than 100bpm • Stretching - reduce DOMS
TABLE 1. ACSM/AHA physical activity recommendations for older adults. 150 min / wk of physical activity for health benefits, additional benefits occur with additional F, I, and T - older adults should be as physically active as their abilities and conditions allow. Frequency: moderate-intensity at least 30 or up to 60 (for greater benefit) min / day in bouts of at least 10 min each to total 150–300 min/wk, at least 20–30 min / day or more of vigorous-intensity activities to total 75–150 min / wk, an equivalent combination of moderate and vigorous activity. Intensity: On a 0 to 10 scale, 5 to 6 for moderate and 7 to 8 for vigorous Duration: For moderate-intensity activities, accumulate at least 30 min/day in bouts of at least 10 min each or at least 20 min/day of continuous activity for vigorous-intensity activities. Type: Any modality that does not impose excessive orthopedic stress; walking is the most common type of activity. Aquatic exercise and stationary cycle exercise may be advantageous for those with limited tolerance for weight bearing activity.
Resistance exercise for older adults: Frequency: At least 2 days / wk Intensity: Between moderate- (5–6) and vigorous- (7–8) intensity on a scale of 0 to 10. Type: Progressive weight training program or weight bearing calisthenics (8–10 exercises involving the major muscle groups of 8–12 repetitions each), stair climbing, and other strengthening activities that use the major muscle groups. Flexibility exercise for older adults: Frequency: At least 2 d/wk. Intensity: Moderate (5–6) intensity on a scale of 0 to 10. Type: Any activities that maintain or increase flexibility using sustained stretches for each major muscle group and static rather than ballistic movements.
Balance exercise for frequent fallers or individuals with mobility problems: Because of a lack of adequate research evidence, there are currently no specific recommendations regarding specific frequency, intensity, or type of balance exercises for older adults. ACSM recommends using activities that include the following: 1) progressively difficult postures that gradually reduce the base of support (e.g.,two-legged stand, semi-tandem stand, tandem stand, one-legged stand), 2) dynamic movements that perturb the center of gravity (e.g., tandem walk, circle turns), 3) stressing postural muscle groups (e.g., heel stands, toe stands), or 4) reducing sensory input (e.g., standing with eyes closed).
The ACSM/AHA Guidelines recommend the following special considerations for older adults. - The intensity and duration of physical activity should be low at the outset for older adults who are highly deconditioned, functionally limited, or have chronic conditions that affect their ability to perform physical tasks. - The progression of activities should be individual and tailored to tolerance and preference; a conservative approach may be necessary for the most deconditioned and physically limited older adults. - Muscle strengthening activities and/or balance training may need to precede aerobic training activities among very frail individuals. - Older adults should exceed the recommended minimums if they desire to improve their fitness. - If chronic conditions preclude activity at the recommended minimum amount, older adults should perform physical activities as tolerated so as to avoid being sedentary.