Download
1 / 66
660 likes | 775 Views
Health Care Reform and the Work of the Super Committee. Peter C. Damiano Director, Public Policy Center University of Iowa. Johnson County Livable Community. November 14, 2011. Today’s Topics . The Patient Protection and Affordable Care Act (PPACA) What is already in place

E N D
Health Care Reform and the Work of the Super Committee • Peter C. Damiano • Director, Public Policy Center • University of Iowa • Johnson County Livable Community • November 14, 2011
Today’s Topics • The Patient Protection and Affordable Care Act (PPACA) • What is already in place • What’s yet to come • ACA and public health • IA Safety Net project • Discussion • What about the Super Committee • What about the Election/Courts
The Patient Protection and Affordable Care Act (PPACA) • Signed into law March 2010 • Emphasis on: • Individual insurance market • Small business insurance market • Few implications for large employer-based insurance • Already self-insured
Market-based reform • Right of center approach to reform: • Similar to proposals by Richard Nixon, Robert Dole and Mitt Romney • Left of center approach-single payer • Uses primarily private insurance companies: Some Gov’t program expansion
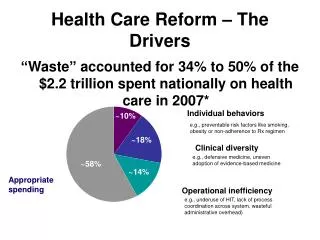
Why Reform Health Care in US • Cost • Access to Care – right vs. privilege • Quality
Coverage in new plan • Net 32 million more insured • Decline of 3 million from employers • Decline of 5 million from non-group 24 million Source: CBO report to Congress, March 2010
Policies Already in Place 25 reforms enacted in 2010 18 of 21 enacted in 2011
Current policies (fall 2010) • Cover children up to 26 on parent’s policies • State/federal high risk pools • Eliminate pre-existing conditions for children • Can’t rescind coverage for illness • Can’t impose yearly and lifetime caps
Current policies (fall 2010) • Small-business tax credits: Small businesses (fewer than 25 employees and average wages under $50,000) that offer health care benefits eligible for tax credits of up to 35% of premiums for 2 years
Current policies (fall 2010) • Establish process to review premium increases • States must report trends in premium increases for inclusion in Exchanges • Establish Center for Medicare and Medicaid Innovation
Current policies (2011) • Discounts to fill doughnut hole • -50% discount on brand name drugs • Minimum Medical Loss Ratios • -requires reporting proportion of dollars spent on clinical services/quality • -must be at least 85% large group • -80% individual and small group • -debate about agent fees
Cost of reform • Total cost: $940 billion first ten years • Impact on deficit: $124 Billion in reductions in the deficit first ten years $1.2 Trillion second ten years Source: Congressional Budget Office, March 2010
Cost of reform • Impact on Medicare/SS solvency: Extend Medicare trust fund solvency 12 years (2017 to 2029) - higher payroll taxes (0.9%) on those making over $200,000 - lower hospital payment rates SS improved by taxing highest benefit plans in 2018 Source: Medicare and Social Security Trustee Report, August 2010
Financing Reform • 10% tax on Indoor Tanning Services • Non-profit hospitals must conduct community needs assessment and develop a financial assistance policy or face $50,000 tax for failure to meet this • Reduced deductions for OTC drugs for Flex or Health Saving Accounts • Reduced deductions for non-medical distributions from Flex or Health Saving Accounts
Future Financing of Reform • Medicare payroll tax on investments (2012): 3.8% on investment income for families >$250,000 • Excise tax on investments (2019): 40% on “Cadillac” plans Source: Congressional Budget Office, March 2010
Future policies (2014) • Individual mandate begins. • Large employer mandate begins (over 50 employees only) • Medicaid expansion begins. • Health insurance Exchanges begin to operate. • Individual • Small businesses
Exchanges generally • Health insurance marketplace (bazaar) • Offer regulated products that meet standards • Require two multi-state plans in each Exchange (federal employee plans) • At least one plan must be offered by a non-profit entity
Coverage for children • Medicaid: up to 133% of FPL • No change for Iowa • CHIP: up to state approved level • 300% FPL in Iowa-no change • Exchange: 300% of FPL and up
Coverage for Adults • Medicaid: up to 133% of FPL • Gets rid of categorical eligibility • Eliminates IowaCare program (probably) • Exchange: 133% of FPL and up
Health Insurance Exchange • American Health Benefit Exchanges • Individuals • 100-200% FPL: $1,983/individual and $3,967/family; • 200-300% FPL: $2,975/individual and $5,950/family; • 300-400% FPL: $3,987/individual and $7,973/family
Health Insurance Exchange • Small Business Health Options Program (SHOP) Exchanges • Up to 100 employees
Preventive coverage • All new group and individual health plans will be required to provide free preventive care for proven preventive services. (2010) • New Medicare prevention coverage (2011)
Public Health and Prevention • $250 million (2010) 4 Activities • Community and Clinical Prevention: $126M • Putting Prevention to Work: $74M • Primary and Behavioral Health Integration: 20M • Obesity Prevention and Fitness:$16M • Tobacco Cessation: $16M • Public Health Infrastructure: $70M • Public Health Infrastructure: $50M • Epidemiology and Lab Capacity: $20M
Public Health and Prevention 2010 • Research and Tracking: $31M • Surveillance: $21M • Community Preventive Services Task Force: $5M • Clinical Preventive Services Task Force: $5M • Public Health Training: $23M • Public Health Workforce: $8M • Public Health Training Centers: $15M
Public Health and Prevention 2011 • National Prevention, Health Promotion and Public Health Council • Senior officials across gov’t agencies • Created by Executive Order June, 2011
Indirect ACA and Public Health issues ACA creates changes and opportunities for safety net providers-currently uncertain environment • Increasing public and private coverage • Funds for FQHCs • Establishment of ACOs • Funds for HIT, HIE, EHRs and meaningful use • Medical home development
Iowa Safety Net, the ACA and Related Primary Care Delivery System Changes
Iowa Safety Net and the ACA Study goal: Use Iowa as a model to inform policymakers about the impact of the ACA and related delivery system changes on safety net providers and payers • Uses Iowa Safety Net Network and national advisory committee to inform process • Emphasis is on primary care • Funded by The Commonwealth Fund with additional support from Wellmark Foundation
Conduct background inventory of safety net providers/payers • Evaluate impact of the ACA as implementation moves forward • Identify opportunities for collaboration and coordination between public and private providers to improve efficiency • Iowa Safety Net and the ACA
Safety net providers • FQHCs • Rural health clinics • Title X funded family planning clinics • Comm. MH/SA centers • Free clinics • Provider Networks/Financing/Patients • Iowa Safety Net and the ACA
Safety net payers • Medicare • Medicaid • CHIP • Title V • Ryan White • Financing/Patients • Iowa Safety Net and the ACA
Major Goals of the Iowa Safety Net Project • Assist policymakers and safety net providers to plan for change-financial and organizational • Conduct large scale strategic planning effort not otherwise possible • Using national and state-level experts with academic assistance to evaluate the potential impacts of ACA on states • Identify opportunities for integration and coordination in the health care delivery system.
Your Concerns, Benefits and Opportunities regarding ACA in Iowa
Your Concerns, Benefits and Opportunities regarding ACA in Iowa
If the ACA does not go through as planned 1) Election2) Supreme Court decision
If the ACA does not go through as planned The 2012 Election
If the ACA does not go through as planned Supreme Court Decision
Supreme court challenge • November 14-Supreme Court said it will hear challenge • Decision likely late June • Focus: • Individual mandate • Jurisdictional issue: can they rule before a tax goes into affect (the fine–1867 Anti-injunction act) • Medicaid expansion and cost to the state • Declined considering penalties to states that they and other employers would face (1985 ruling that states must comply with employer-related laws)
Lower court rulings • 30 lawsuits have been filed • Half of the states have filed briefs against ACA • Federal appeals courts (four rulings): • Commerce clause at issue • Two upheld the law • One ruling it unconstitutional • One saying ruling premature (not in place) • Social security, civil rights acts, tax power Supreme court case from: • National Federation of Independent Business v. Sebelius, 11-393; Department of Health and Human Services v. Florida, 11-398; and Florida v. Department of Health and Human Services, 11-400.
DC Court of Appeal Ruling November 7, 2011 ruling • Majority opinion: Laurence H. Silberman • 2-1 in support of individual mandate “The right to be free from federal regulation is not absolute, and yields to the imperative that Congress be free to forge national solutions to national problems, no matter how local — or seemingly passive — their individual origins,” he wrote. The fact that Congress may have never issued an individual mandate to purchase something before, a central argument for many opposing the law, “seems to us a political judgment rather than a recognition of constitutional limitations,” NY Times, Nov. 8, 2011