Download
1 / 44
590 likes | 992 Views
ALLHAT. Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210. ALLHAT. Introduction and Background.

E N D
ALLHAT Role of Diureticsin the Prevention of Heart Failure -The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
ALLHAT Introduction and Background • Heart failure is a major public health problem, especially in persons 65 years of age and older (= number one reason for hospitalizations in this age group). • Age-adjusted incidence per 100,000 person-years during 1990-1999 was 564 for men and 327 for women, age 65-74 years (NEJM, 2002, Framingham) • Five-year age-adjusted survival rate was only 59% among men and 45% for women. • In 91% of HF cases, hypertension is an antecedent (Framingham, JAMA, 1996)
ALLHAT Hypertension Controland Heart Failure • In a meta-analysis of 12 trials of patients with hypertension it was found that, compared to placebo, drug therapy for hypertension prevents over 50% of HF events (Moser, JACC, 1996). • In another meta-analysis, diuretics and beta-blockers (BB) were equally effective in preventing HF events (Psaty, JAMA, 1997).
ALLHAT Hypertension Controland Heart Failure • A meta–analysis of active comparator trials found no significant difference between ACE-inhibitors and diuretics for preventing HF; ACE-inhibitors were more efficacious than CCBs (BPLTT Collaboration, Lancet, 2002). • The INSIGHT trial found that a long-acting nifedipine regimen was associated with a > 2x higher incidence of HF events compared to a diuretic combination (HCTZ/amiolride) (Brown, Lancet, 2000).
ALLHAT Objectives • Characterize HF in ALLHAT by its antecedent risk factors and underlying conditions. • Examine occurrence of HF by treatment group overall, in subgroups, and over time. • Explore relation of initial occurrence of HF to pre-randomization type of BP medication used. • Explore follow-up BP and use of additional drugs as mediating/modifying factors. • Examine post-HF mortality overall and by treatment group.
ALLHAT Randomized Design of ALLHAT Hypertension Trial 42,418 high-risk hypertensive patients 90% previously treated 10% untreated STEP 1 AGENTS Chlorthalidone 12.5-25 mg Lisinopril 10-40 mg Doxazosin 1-8 mg Amlodipine 2.5-10 mg N=9,061 N=9,054 N=9,048 N=15,255 Other AHT Drugs STEP 2 AND 3 AGENTS (5 years) Atenolol 28.0% Clonidine 10.6% Reserpine 4.3% Hydralazine 10.9%
ALLHAT Decision to StopDoxazosin Arm • NHLBI Director accepted recommendation of independent review group to terminate doxazosin arm (early in year 2000), due to: • Futility of finding a significant difference for primary outcome • Statistically significant 25 percent higher rate of major secondary endpoint, combined CVD outcomes, along with twofold higher rate of HF • Detailed HF analyses published (Davis et al. Ann Intern Med 2002).
ALLHAT Heart Failure Data Collection • Hospitalized nonfatal – discharge summary • Hospitalized fatal – death certificate, discharge summary • Nonhospitalized fatal – death certificate • Nonhospitalized nonfatal (treated) – clinician report • 100% review of discharge summaries and death certificates by CTC Medical Reviewers • Queries to clinics if diagnosis questionable
ALLHAT ALLHAT Criteria for HF Evaluation* *ALLHAT Manual of Operations, 5.3.4; adopted from the SHEP trial
ALLHAT Validity of HFOutcome Verified • Traditional risk factors in agreement with previous studies, e.g., Framingham • HF Validation Study confirmed original observed treatment differences • Independent central review using both ALLHAT and Framingham criteria
ALLHAT Heart FailureValidation Study
ALLHAT Inclusion/Exclusion Criteria for Antihypertensive Trial • Men and women > 55 years old • If untreated: 140/90, 180/110 mm Hg (2 visits) • If treated: ≤ 160/100 mm Hg (visit 1), ≤ 180/110 mm Hg (visit 2) • No washout required • At least one additional cardiovascular risk factor • Exclude if symptomatic HF or EF < 35%, creatinine 2 mg/dL, require diuretics, CCB, ACEI, or AB’s for non-BP indication
ALLHAT Step 1Treatment Protocol Step 2/3 drugs –– atenolol, reserpine, clonidine, hydralazine “Non-study” drugs –– all other antihypertensive medications
Baseline Characteristics ALLHAT
ALLHAT Hospitalized/ Fatal Heart Failure by ALLHAT Treatment Group .1 .08 Chlorthalidone Amlodipine Lisinopril .06 Cumulative Event Rate .04 .02 0 0 1 2 3 4 5 6 7 Years
ALLHAT Heart Failure Before and After 1 Year • Observed HF differences were larger earlier in the follow-up. • The lisinopril group had a lower HF rate than the amlodipine group, but event curves did not separate until later. • A test of the proportional hazards assumption for Cox regression revealed that RRs were not constant over time. Therefore, a Cox regression that used a time-dependent indicator variable (<=1 year versus >1 year) was utilized.
ALLHAT Chlorthalidone Amlodipine Lisinopril Hospitalized/ Fatal Heart Failure by ALLHAT Treatment Group Within 1 Year and >1 Year .1 .02 .08 .06 Cumulative Hosp/Fatal HF Rate .01 .04 .02 0 0 0 1 2 3 4 5 6 7 0 .5 1 Years to Hosp/Fatal HF Years to Hosp/Fatal HF
ALLHAT Hospitalized/fatal HF in Subgroups - Amlodipine / Chlorthalidone Relative Risks from Baseline to 1 Year of Follow-up Relative Risk (95% CI) Favors Amlodipine Favors Chlorthalidone Total 2.22 (1.69 - 2.91) Age < 65 2.89 (1.62 - 5.17) Age ≥ 65 2.06 (1.51 - 2.80) Non-Black 2.12 (1.49 - 3.01) Black 2.37 (1.55 - 3.63) Men 2.27 (1.56 - 3.30) Women 2.17 (1.46 - 3.21) Diabetic 2.71 (1.83 - 4.02) Non-Diabetic 1.83 (1.25 - 2.67) 0.50 1 2 3 4 5 6
ALLHAT Hospitalized/fatal HF in Subgroups - Amlodipine / Chlorthalidone Relative Risks After 1 Year of Follow-up Relative Risk (95% CI) Favors Amlodipine Favors Chlorthalidone Total 1.22 (1.08 - 1.38) Age < 65 1.38 (1.10 - 1.73) Age ≥ 65 1.17 (1.02 - 1.35) Non-Black 1.20 (1.04 - 1.39) Black 1.28 (1.03 - 1.58) Men 1.28 (1.09 - 1.50) Women 1.16 (0.97 - 1.39) Diabetic 1.23 (1.04 - 1.46) Non-Diabetic 1.21 (1.02 - 1.43) 0.50 1 2 3 4 5 6
ALLHAT Hospitalized/fatal HF in Subgroups - Lisinopril / Chlorthalidone Relative Risks from Baseline to 1 Year of Follow-up Relative Risk (95% CI) Favors Lisinopril Favors Chlorthalidone Total 2.08 (1.58 - 2.74) Age < 65 2.53 (1.39 - 4.59) Age ≥ 65 1.98 (1.45 - 2.70) Non-Black 2.04 (1.43 - 2.90) Black 2.15 (1.39 - 3.33) Men 1.80 (1.22 - 2.67) Women 2.40 (1.63 - 3.54) Diabetic 1.99 (1.31 - 3.05) Non-Diabetic 2.16 (1.50 - 3.10) 0.50 1 2 3 4 5
ALLHAT 0.96 (0.85 - 1.10) 0.95 (0.74 - 1.23) 0.97 (0.84 - 1.13) 0.90 (0.77 - 1.06) 1.10 (0.88 - 1.37) Total 1.02 (0.86 - 1.21) Age < 65 0.89 (0.73 - 1.09) Age ≥ 65 1.01 (0.84 - 1.22) Non-Black 0.93 (0.77 - 1.12) Black Men Women Diabetic Non-Diabetic Hospitalized/fatal HF in Subgroups - Lisinopril / Chlorthalidone Relative Risks After 1 Year of Follow-up Relative Risk (95% CI) Favors Lisinopril Favors Chlorthalidone 0.50 1 2
ALLHAT HF Development and Relation to Other Outcomes • HF development associated with: • 6.6-fold increase in death rate • 11.7-fold increase in CV death rate • Previous MI → 5.7-fold increased HF risk • Of participants with hospitalized HF: • 72% hospitalized once • 23.3% hospitalized 2-3 times • 4.7% hospitalized 4+ times
ALLHAT Why are hazard ratios not constant throughout? Hypotheses? • Withdrawal from BP meds used prior to enrollment • Time course for effect of first-step (primary) drug • Diuretic – immediate? • ACEI – delayed? • Addition of step-up meds (esp. anti-HF meds) • Differences in BP
ALLHAT Prior Use ofAntihypertensive Agents • Prior medication use associated with HF risk, especially during first year • RR 1.42 (1.18 – 1.71) • Relative benefits of chlorthalidone consistent with or without prior antihypertensive medication use
ALLHAT Specific PriorAntihypertensive Agents • Data not collected within ALLHAT • Available for 1115 / 1773 HF cases • Case-only analysis • No evidence for any statistically significant interaction between prior drug type (e.g., diuretic) and treatment effect for HF, overall or during the first year
ALLHAT Immediate vsDelayed Effects • Do diuretics have a more immediate effect on HF prevention than ACEI or ARB? • Effect of diuretics begins at trial onset • Several ACEI vs placebo studies suggest that ACEI effect is not immediate • VALUE trial – valsartan vs amlodipine – HF similar in first 2 years, strong trend afterward favoring valsartan
ALLHAT Use of Step-upBP Meds Addition of Step 2 and Step 3 meds could have contributed to lessening or cessation of divergence of HF curves after 1 year.
Diuretic, ACEI,or Atenol Use ALLHAT
ALLHAT BP Results by Treatment Group Compared to chlorthalidone: SBP significantly higher in the amlodipine group (~1 mm Hg) and the lisinopril group (~2 mm Hg). Compared to chlorthalidone: DBP significantly lower in the amlodipine group (~1 mm Hg).
ALLHAT BP Differences • Adjustment for follow-up SBP as time-dependent covariates in a Cox regression model only slightly modified the relative risks • Amlodipine/chlorthalidone 2.22 2.16 first year, 1.22 1.18 after 1 year • Lisinopril/chlorthalidone 2.08 2.01 first year, 0.96 0.93 after 1 year
ALLHAT All-Cause Mortality Chlorthalidone Amlodipine Lisinopril .6 .5 .4 Cumulative Event Rate .3 .2 .1 0 0 1 2 3 4 5 6 7 Years from Hospitalized HF to Death
ALLHAT Post-HF Mortality • Mortality rates after hospitalized HF high relative to those seen in ALLHAT overall • 25% vs 5% at 2.5 years, respectively • No significant treatment group differences for post-HF mortality • The reason that the treatment difference for hospitalized HF did not translate into an effect on total mortality is that only 5.6% of all deaths were attributed to HF.
ALLHAT Heart Failureand Total Mortality • Lisinopril-chlorthalidone absolute difference in hospitalized HF over 6 years was 0.4%. • The excess of cases in the lisinopril group = 36 patients. • Case-fatality rate over average follow-up of 2.5 years = 25%. • Thus, 9 excess cases of fatal HF would be expected in the lisinopril group. This is fewer than 1% of all deaths in the lisinopril group (n=1314). • Similar calculations for the amlodipine group: • 154 excess cases of hospitalized HF • Estimated number of fatal HF cases was 39, 3% of the amlodipine deaths (n=1256).
ALLHAT Effect on Total Mortality • HF differences in the trial would not have affected differences in total mortality • Also noted in the BPLTTC analyses • Absolute HF risk low • Increase in RR outweighed by even small reduction in higher absolute risks for stroke and CHD • Differences in # of HF events during trial result in only very small differences in # of deaths • ALLHAT post-trial mortality surveillance to examine this further
ALLHAT Conclusions 1 • Chlorthalidone superior to amlodipine in both time periods • Chlorthalidone superior to lisinopril during the first year • True for subgroups – age, race, sex, diabetes history • Other factors could not individually account for all of the observed treatment differences • Prior antihypertensive meds • Other open-label BP meds • Follow-up BP differences
ALLHAT Conclusions 2 • Developing HF is associated with a high mortality rate (~50% at 5 years) • It may take time for HF differences to translate into detectable mortality differences between treatments • Diuretics are clearly preferred over CCBs overall and over ACE inhibitors, at least in the short term, in preventing HF.
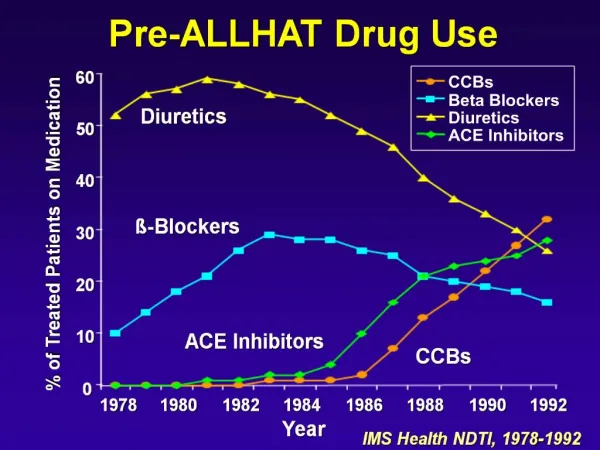
ALLHAT Placebo-Controlled Trials • Most placebo-controlled trial have used diuretics and/or β-blockers as active regimens • Diuretics & ACEI shown to prevent HF in patients with hypertension • SHEP, HOPE • CCB vs placebo trials less conclusive • Syst-Eur • Meta-analyses – active therapy of hypertension can prevent >40% of HF events • Psaty, Smith, Siscovick, et al.
ALLHAT Active-Controlled Trials • VALUE • STOP Hypertension-2 • ANBP2 • INVEST • CONVINCE – CCB or diuretic/β-blocker • BP reduced similarly, HF 30% more with CCB
ALLHAT BPLTTC Meta-Analyses • CCB-based therapies • NS 20% increase in HF incidence compared with placebo • 33% higher risk of HF compared with diuretic/β-blocker • ACEI-based therapies • 18% fewer HF events than with CCB or placebo • 7% NS higher risk than with diuretic/ β-blocker • CCBs less effective in preventing HF than other regimens • ACEI no more effective in preventing HF than diuretic/ β-blocker
ALLHAT Randomized Designof ALLHAT Amlodipine Chlorthalidone Doxazosin Lisinopril High-risk hypertensive patients ≥ 55 years Consent / Randomize (42,418) Eligible for lipid-lowering Not eligible for lipid-lowering Consent / Randomize (10,355) Pravastatin Usual care Follow for CHD and other outcomes until death or end of study (up to 8 yr).
Event Reduction in SHEP, Syst-Eur, and HOPE SHEP: Systolic Hypertension in the Elderly, n=4,736;chlorthalidone Syst-Eur: Systolic Hypertension in Europe, n=4,695;nitrendipine HOPE: Heart Outcomes Prevention Evaluation Study, n=9,297;ramipril