Download
1 / 18
190 likes | 205 Views
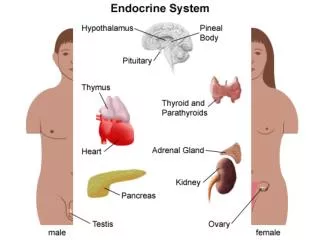
Endocrine Complication in Thalassaemia Major: Growth & Puberty. Dr Wong Lap Ming Department of Paediatrics & Adolescent Medicine Tuen Mun Hospital 15-7-2004.

E N D
Endocrine Complication in Thalassaemia Major:Growth & Puberty Dr Wong Lap Ming Department of Paediatrics & Adolescent Medicine Tuen Mun Hospital 15-7-2004
Iron overload leads to formation of free radicals which damage membrane lipids and other macromolecules, leading to cellular damage and necrosis.
Prevalence of endocrine disturbance in 165 patients with thalassaemia major* • Secondary amenorrhoea 50% • Hypogonadotrophic hypogonadism 43% • Short stature 34% • Impaired glucose tolerance 24.7% • IDDM 18.8% • Primary hypothyroidism 9% • GH deficiency/insufficiency 6% • Hypoparathyroidism 5% • * De Sanctis. Growth and Puberty and its Management in Thalassaemia. Horm Res 2002;58(suppl 1):72-79
Causes of short stature • Chronic anaemia, hypersplenism, folate deficiency. • Endocrine disturbance owing to iron overload ( Growth hormone axis, hypothyroidism & hypogonadism) • Chronic liver disease • Bone dysplasia owing to desferrioxamine # Diminished spinal growth mainly accounts for the short stature.
Iron concentration per gram of liver dry weight < 3mg risk of toxicity owing to chelating agent 5-15mg risk of organ damage >15mg cardiomyopathy & death
Desferrioxamine toxicity • Desferrioxamine inhibit DNA synthesis, fibroblast proliferation, collagen formation & zinc deficiency. • Bone dysplasia manifested as bone pain, back pain, limited joint movement, reduction in height velocity, platyspondylosis (short spine), widened growth plate ( especiallly in wrist & knee).
Desferrioxamine toxicity, radiological changes • Thickened growth plate with widening & cupping of metaphysis • Sclerosis of sub-chondral bone with small radiolucent areas in metaphyses. • Osteoporosis & increased trabecular pattern of long bones.
Zinc deficiency Growth retardation Delayed bone maturation Hypogonadism
Growth pattern of thalassaemia major • Childhood : normal height velocity • 8-9 years : decreased height velocity • Pubertal : absent or suppressed growth spurt * There is decreasing upper to lower segment ratio during puberty as a result of diminished spinal growth. * Height gain can be prolonged until 20s, but the final height is often more than 2.5SD below the mean.
GH axis disturbance (1) • High/normal/reduced GH response to stimulation test • Reduced spontaneous secretion (neurosecretory dysfunction) • Low IGF-1 level despite normal GH level ( owing to liver disease) • Treatment with GH is with variable success, depending on underlying cause for the short stature.
GH axis disturbance (2) • The low IGF-1 in short patient with GH reserve suggested defect in GH-receptor or post-receptor abnormality. • Supra-physiological doses of GH resulted in sub-normal rise in IGF-1 level suggesting that short stature might not be corrected by GH treatment.
Suggested management approach* • Investigations Auxology: standing & sitting height, pubertal stage Bone age GH stimulation test, IGF-1 & IGFBP-3 if available TSH, fT4 R/LFT CaPo, serum zinc, serum ferritin * Wonke B, De Sanctis V. Haemoglobinopathies. In Kelnar CJ, Savage MO, Stirling HF, Saenger P. Growth disorders,pathophysiology and treatment. Chapman & Hall Medical, 1998:471-482.
Suggested management approach* • Recombinant human GH ( 0.6-0.8 IU/kg per week in pre-pubertal, 0.9 IU/kg per in pubertal) Responder: height velocity >4cm/yr greater than previous yr. Partial responder: height velocity 2-4cm/yr greater than previous yr Non-responder: height velocity <2cm greater than previous yr * Final height gain remains uncertain. ** Wonke B, De Sanctis V. Haemoglobinopathies. In Kelnar CJ, Savage MO, Stirling HF, Saenger P. Growth disorders,pathophysiology and treatment. Chapman & Hall Medical, 1998:471-482.
Hypogonadism • The most common endocrine disturbance. • Causes: Pituitary gonadotrophs damage Gonadal damage Liver disease Chronic hypoxia DM Zinc deficiency
Evidence of pituitary damage • Histological finding of reduced numbers of cells. • Selective iron deposition in gonadotrophic cells • Mean Pituitary volume lower as detected by MRI. • Reversal of hypogonadotrophic hypogonadism after removal of iron overload is rare. • In contrast, iron deposition in gonads do not have a significant negative effect on function.
Presentation • Female: poor/absent breast development, delayed menarche, oligomenorrhoea or secondary amenorrhoea. • Male: failure of testicular and penile enlargement,sparse facial and body hair, decreased libido.
Assessment • Auxology: standing & sitting height, pubertal stage, bone age. • Serum LH & FSH before & after GnRH stimulation. • Serum estradiol & testosterone.
Induction of puberty • Female: (may start at chronological age of 13, bone age of 10-11 yr) Ethinylestradiol 2.5-5 mcg daily for 3-6 months. If there is no evidence of biochemical pubertal progress, a gradual increase of sex steroid is recommended , follows by cyclical estrogen & progesterone. • Male: Sustanon 25-50 mg per month for 3-6 months. If puberty does not progress spontaneously, treatment is continued with gradual increase in dose.