Download
1 / 103
1.04k likes | 1.25k Views
Problematic Compliance Issues Identified by The Joint Commission and CMS. Dale Brown, RN, MSN Principal Consultant Kent & Associates Knoxville, Tennessee. Accreditation Decisions. Preliminary Accreditation Accredited Accredited with follow-up survey (30 days to 6 months) (Non-CMS issues)

E N D
Problematic Compliance Issues Identified by The Joint Commission and CMS Dale Brown, RN, MSN Principal Consultant Kent & Associates Knoxville, Tennessee
Accreditation Decisions • Preliminary Accreditation • Accredited • Accredited with follow-up survey (30 days to 6 months) (Non-CMS issues) • Contingent Accreditation: follow up survey within 30 days • Preliminary Denial • Denial
Flow of Decision • Accreditation with follow-up survey (1st failed condition level deficiency) • Contingent accreditation (2nd failed CLD) • PDA: Immediate threat to life
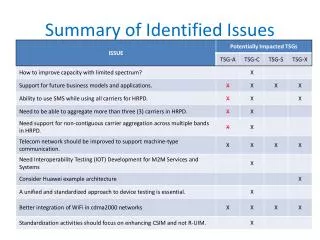
Flow of Decision • Single or multiple instances • Nature and significance of findings • Failed On-site ESC • Decision rules triggered • Repeat findings
Condition Level Deficiencies • Determination based on manner and degree: • Manner: prevalence, how pervasive, number frequency • Degree: magnitude, how severe, how bad • Collaboration among team members AND Central office staff
Survey Process Changes • Minimum of 30 records or 10% of ADC whichever is greater. • Small hospitals with ADC less than 20, then 20 records • Small hospital exception does not apply to specialty hospitals.
Condition Level Deficiencies • Noncompliance within the condition stem statement • Single requirement out of compliance which is of such magnitude to result in noncompliance with entire condition • Many requirements and standards noncompliant
Condition Level Deficiencies • Follow up survey MUST occur within 45 calendar days of last day of accreditation survey • If the problem remains a second follow up survey MUST occur within 30 days of first follow up survey
Condition Level Deficiencies • The follow up survey will focus on the RFIs that were determined to be the condition level deficiencies • The surveyors can score other issues that are identified during an onsite visit • Failure to clear a condition level deficiency after the second survey results in notification to CMS
Condition Level Deficiencies • Governing Body CoP: • When any condition level deficiencies are identified during the survey, The Joint Commission is required to include a condition level deficiency in the leadership standards.
Scoring/Decision • The frequency of “Bulleted” points has been reduced. • Elements of Performance and other accreditation requirements will be tagged based on their “criticality” – immediacy of the impact on quality of care and patient safety as the result of noncompliance. • – Direct Impact requirements. • – Indirect Impact requirements.
Scoring/Decision • Potentially multiple submission deadlines based on the “immediacy” of risk. • – Direct Impact Requirements: ESC due within 45 days. • – Indirect Impact Requirements: ESC due within 60 days.
Scoring/Decision • Partial compliance • Insufficient compliance is not resolved
Progressively More Adverse Accreditation contingent preliminary denial of accreditation provisional
Scoring/Decision • The Immediate Threat to Life process has been modified. Upon resolution of the threat, the accreditation status will change from Preliminary Denial of Accreditation (PDA) to Contingent Accreditation and include a follow-up survey.
Scoring/Decision • The report which is presented to the organization at the conclusion of the survey will be modified, as follows: • 1. Title changed to – “Summary of Survey Findings” • 2. The report is now sorted by chapters in the applicable Accreditation Manuals
Scoring/Decision • 3. The content includes the standards, elements of performance, and other accreditation requirements which have been found to be less than fully compliant at the time of survey, as well as the associated survey team observations.
Scoring/Decision • 4. The report does not include a potential accreditation decision. The “official” version of the report which is posted to the organization’s extranet site post-survey will contain the potential accreditation decision. • 5. The report will no longer include “Supplemental Findings” • Name of the survey team is no longer included
Scoring/Decision “Immediate Threat to Life” PDA “Situational Decision Rule” Conditional or PDA “Direct Impact Standards” Shorter time frame “Indirect Impact Standards” Longer time frame
Immediate Threat to Life • Situations, identified at the time of survey, which have or may potentially have a serious adverse effect on patient health and safety. • The Joint Commission President can issue an expedited Preliminary Denial of Accreditation (PDA) decision.
Immediate Threat to Life • PDA remains until corrective action is demonstrated, via an on-site validation survey. • PDA changes to Contingent Accreditation which includes a follow-up survey to assess sustained implementation
Situational Decision Rule • Examples: • Unlicensed facility • Unlicensed individual who requires a license • Failure to implement LSC deficiencies • Some standards will trigger a situational decision rule directly and immediately
Joint CommissionCMS Relationship TJC CMS
TJC-CMS • CMS requires accreditation to participate in Medicare and Medicaid programs. • Accreditation can be granted by CMS, States surveying on behalf of CMS, TJC, HFAB, or DNV.
TJC-CMS • CMS issues Conditions of Participation. These are regulatory and compliance is not optional. • In order to be accredited, hospitals must comply with CMS Conditions of Participation.
TJC-CMS • By having a Joint Commission survey, Joint Commission is “deeming” the hospital to be compliant with CMS. • Not all Joint Commission standards are required by CMS. • Not all CMS Conditions of Participation are reflected in Joint Commission standards.
TJC-CMS • Recently Joint Commission has had to release new standards to more closely align itself with CMS, but the revisions are not complete. • Most CMS related TJC standards are “A” elements of performance, requiring 100% compliance.
TJC-CMS • If hospitals are found to be non-compliant at a standards level, accreditation can still be awarded. • If hospitals are found non-compliant at a “Condition Level”, then there must be an additional CMS and Joint Commission follow up survey.
TJC-CMS • Much focus in consulting is now on CMS in addition to Joint Commission compliance. • Hospitals must always be aware that reporting to external agencies occurs, including CMS, and DEA. • Condition level citations will result in a follow up survey.
Three Year Surveys • As of January 2011, all surveys will be conducted within a 3 year period (36 months from the last survey) rather than 39 months which was the previous practice. • Laboratory surveys will be continue to be conducted 24 months from the previous survey. 2015 2012
Revised Joint Commission Standards to Align with CMS TJC CMS
Changes to reflect the COP • Selected standards were revised to meet relevant Conditions of Participation (CMS) for psychiatric hospitals who use the Joint Commission for Deemed Status which became effective February 1, 2011. • Standards involved EC. 02.03.01, EC. 02.05.03, Emergency Management (EM 03.01.03), Information Management ( IM. 02.02.03), Leadership( 04.01.05), Life Safety Code (LS. 02.01.30), Provision of Care (PC 01.02.13, PC 01.03.01).
Environment of Care EC. 02.03.01-Managing Fire Risks • Applicable to Hospitals and Critical Access Hospitals • The organization must have a written fire plan ( LS. 02.01.70, EP. 4) • Cross referencing to the roles of staff, when and how to sound fire alarms , how to contain smoke and fire, fire extinguisher use and evacuation are also referenced at (EC. 03.01.01, EP.2 & HR. 01.04.01, EP 2)
Environment of CareEC.02.05.03-Reliable Emergency Electrical Power Source • EP’s 1-6 modified to reflect the change of the NFPA’99, 1999 edition (Section 12-3.3) versus Section 13-3.3
Emergency Management EM 03.01.03 • Special Note # 4- In order to satisfy the twice-a-year requirement, the hospital must first evaluate the performance of the previous exercise and make any needed modification to its Emergency Operations plan before conducting the subsequent exercise in accordance with the EP’s 13-17.
Information ManagementIM 02.02.03 • The hospital retrieves, disseminates, and transmits health information in useful formats. • Revision: Hospitals that use CMS for deeming –The medical records system allows for timely retrieval of patient information by diagnosis and procedure.
Leadership LD. 04.01.05 • The hospital effectively manages its programs, services, sites or departments. • EP # 10 for those psychiatric hospitals that use the Joint Commission for deemed status must comply with having a Director of Social Work who monitors and evaluates the social work services furnished.
Life Safety CodeLS. 02.01.30 • The note for EP # 6 was removed as follows: Unsealed spaces 1/8 inch wide or less around pipes, conduits, ducts and wires above the ceiling are permitted. • The note for EP # 25 was removed as follows: For The Joint Commission/s accepted amount of alcohol based hand rub permitted within a single smoke compartment was changed to http://www.jointcommisison.org/assets/1/18/acceptable%20practices%20of%20using%20Alcohol2.pdf
Provision of CarePC. 01.02.13 • EP # 2- For psychiatric hospitals that use Joint Commission standards for Deemed Status purposes: Patient’s who receive treatment for emotional and behavioral disorders receive an assessment that includes the following : The reason for admission as stated by the patient and/or others significantly involved in the patient’s care.
Provision of CarePC. 01.02.13 • EP # 6- For psychiatric hospitals that use Joint Commission standards for Deemed Status purposes: Based on the patient’s age and needs, the assessment for patients who receive treatment for emotional and behavioral disorders include the following: A complete neurological examination when indicated.
Provision of CarePC. 01.03.01-Planning Care • EP. # 5-For psychiatric hospitals that use Joint Commission standards for Deemed Status purposes: The written plan of care is based on patient’s goals and the time frames, setting, and services required to meet those goals. The patient’s goals include both short-term and long-term goals. • EP. #43-The plan of care includes the responsibilities of each member of the treatment team.
EC. 02.03.05Maintenance of Fire Safety Equipment • Changes will be in effect July 1, 2011 unless otherwise dictated by CMS. • For hospitals using the Joint Commission for Deemed status purposes: • EP # 2-At least quarterly the hospital tests water-flow devices. (Was every 6 months)
EC. 02.03.05Maintenance of Fire Safety Equipment • EP # 25-Documentation of maintenance, testing, and inspection activities for fire alarm and water-based fire protection systems includes the following: • Name of the activity • Date of the activity • Required frequency of the activity • Name and contact information, including affiliation of the person who performed the activity • Results of the activity.
EC. 02.03.05Maintenance of Fire Safety Equipment • Additional guidance may be found at NFPA 24, 1998 edition (Section2-1.3) and NFPA 72. 1999 Edition (Section 7-5.2)
CMS New Department Requirements
RADIOLOGY • New CMS requirements for oversight of radiology. • Policies and procedures must comply with nationally recognized standards: ACR • Physician supervision of all contrast administration (CT and MRI). • Physician must be permitted by director of radiology to use radiology equipment.
RADIOLOGY • Training of all providers who operate radiology equipment: physicians and staff using C-Arm, Fluoroscopy.