Download
1 / 96
1.01k likes | 2.64k Views
Mucinoses, Lichen Planus and Related Conditions . Adam Wray, D.O. September 28, 2004. What is Mucin?. Fibrillar matrix in dermis called ground substance, created by fibroblasts.

E N D
Mucinoses, Lichen Planus and Related Conditions Adam Wray, D.O. September 28, 2004
What is Mucin? • Fibrillar matrix in dermis called ground substance, created by fibroblasts. • GS= acid glycosaminoglycans (formerly called acid mucopolysaccharides) that bind 1000 times their own volume in water • Adding sulfates to the acid GAGs creates chondroitin sulfate and dermatan sulfate, the 2 primary dermal mucins
Classification • Primary mucinoses • Mucin deposition is the main histologic feature • Secondary mucinoses • Mucin deposition is an additional finding
H&E: GA: Wispy bluish, feathery material between collagen bundles
Mucin Stains • Colloidal Iron • Alcian Blue • Toluidine Blue • Incubation of tissue in hyaluronidase eliminates the staining, confirming the presence of mucin
Lichen Myxedematosus • Aka Papular Mucinosis • Generalized = Scleromyxedema • Onset age 30-80 • Multiple waxy 2-4mm dome shaped or flat topped papules, usu. linear array • Acral: dorsal hands, face, elbows, and extensor extremities
Acral Persistent Papular Mucinosis • Subtype of localized LM • Usually women • Few to 100 bilaterally symmetrical 2 to 5mm, flesh colored papules • Always on hands and wrists. • Rarely elbows and knees • No paraprotein, no systemic dz • H&E: Increased mucin, but not fibroblasts
Cutaneous Mucinosis of Infancy • Subtype of localized LM • 3 cases, onset birth-3 months of age • 2-8mm papules trunk, extremities, especially backs of hands • TSH, Paraprotein negative • There are neither systemic symptoms nor spontaneous resolution • H&E: papillary dermal mucin, no fibroblasts
Histopathology of lichen myxedematosus (discrete type). Mucin deposits splay collagen bundles in the dermis, but there is only slight fibroblast proliferation and no sclerosis.
Lichen myxedematosus of the discrete type demonstrating mucin accumulation in the dermis. Alcian blue stain (pH 2.5).
Scleromyxedema • Woody, fibrous sclerosis of skin • Lesions coalesce to form leonine facies • Decreased ROM of hands, lips and extremities • Dysphagia is most common GI symptom
Scleromyxedema: Systemic • Pulmonary • Proximal Muscle weakness • Carpal Tunnel Synd. • Peripheral Neurop. • Raynauds • IgG lambda paraproteinemia • Myeloma
Scleromyxedema • Widespread eruption of 2-3 mm, firm, waxy, closely spaced papules • Papules often arranged in a linear array • Surrounding skin is shiny and indurated (sclerodermoid) • “Doughnut sign” = central depression surrounded by an elevated rim (due to skin thickening) is seen on the PIP joints.
Scleromyxedema: Histopathology • Triad • Diffuse deposit of mucin in the upper and mid-reticular dermis • Increase in collagen deposition • Marked proliferation of irregularly arranged fibroblasts
Differential diagnosis • Granuloma annulare • Lichen amyloidosis • Lichen planus • Eruptive collagenoma • Systemic scleroderma • Scleredema
Treatment • Oral retinoids • Systemic corticosteroids • Extracorporeal photochemotherapy • Melaphan • Topical and intralesional hyaluronidase • Electron-beam radiation • Plasmapharesis • PUVA • Dermabrasion • Topical DMSO • Overall prognosis is poor.
Papular Mucinosis and AIDS • Widespread • Not associated with a paraprotein • Always seen in advanced HIV disease • If assoc. with eczematoid dermatitis, clears when eczema clears • Oral retinoids
Scleredema • Stiffening and hardening of the subcutaneous tissues as if they were infiltrated with paraffin. • With DM II (men); without DM II (women) • Begins on the neck, may spread symmetrically to arms, shoulders and back • Skin waxy, wood-like. • Demarcation poor if no DM, good if DM
Scleredema without DM II • F>M 2:1, Poorly demarcated edges • 25% Streptococcal infection • Paraproteinemia usually IgG, Myeloma • Cardiac arrhythmias. • Upper GI dysphagia, tongue involvement • Pleural, pericardial or peritoneal effusion • If infection precedes it, 50% resolve 2-3 yrs.
Scleredema with DM II • Most common, well demarcated edges • M>F 10:1, usually obese • Sharp step off at lesion edge • Persistent erythema & folliculitis possible • Controlling DM II has no effect on skin • No visceral disease or paraprotein
Treatment • PUVA • Pulse therapy with cyclophosphamide and corticosteroids • Electron-beam therapy • Cyclosporine • Therapy has little benefit, however • Systemic and intralesional steroids, intralesional hyaluronidase, MTX, antibx, and penicillamine have not proved helpful
REM Syndrome • Reticular Erythematous Mucinosis • Aka Plaque-like Cutaneous Mucinosis • Women, 3rd -4th decades of life • Frequently follows intense sun exposure, and often pregnancy, OCPs, menses • DIF, ANA negative • MC midline chest & back • Reticulate or plaque-like appearance • Antimalarials often helpful
Cutaneous Focal Mucinosis • Benign, symptomless, skin colored solitary lesions less than 1 cm • Resemble neurofibromas, cyst, BCC, and angiomyxoma • Can occur anywhere on the the body, except over the joints of the hands and feet • Adulthood • Histopath: mucin throughout upper and mid-dermis sparing subQ fat. Cleft like spaces, but no cysts, are seen. Numerous vimentin-positive dendritic shaped fibroblasts are seen • Tx: Surgical excision
Self-healing Juvenile Cutaneous Mucinosis • Sudden onset, age 5 to 15 • Skin lesions and polyarthritis x a few mos. • Ivory white papules head, neck, trunk and periarticular • Hard edema of periorbital area/face • TSH, IgG normal • H&E dermal mucin • Prognosis excellent
Follicular Mucinosis • Aka Alopecia Mucinosa, 3 groups • MC young, head, neck arms, resolves in 2 mos to 2 years • 2nd group, larger more numerous lesions, takes several years to resolve • 3rd group, older, CTLC • 30% of FM patients have MF • Any patient >30 yo with FM, look for MF
Follicular papules merging into a scaly plaque with alopecia
MF associated follicular mucinosis H&E: asterisks mark large collections of mucin within cells of the sebaceous gland and outer root sheath with mixed dermal infiltrate
Treatments for Follicular Mucinosis after you have ruled out MF: • Topical or oral corticosteroids • Dapsone • PUVA, Radiation therapy • Interferon alfa-2b • Mepacrine • Indomethacin • Minocycline • Oral isotretinoin
Myxoid Cysts • MC terminal dorsal or lateral fingers • Solitary 5-7mm opalescent or skin colored asymptomatic swellings of proximal nail fold or DIP • NO CYSTIC LINING, not a true cyst • Synovial origin still debated • TX: I&D, Cryo, IL steroids, Fulguration of the base after draining. Meticulous excision including “stalk” by Salasche in 11 pts, no recur.
Groove of nail plate secondary to lesional pressure to the nail matrix
Case of dermatomyositis presenting with cutaneous mucinosis as the sole manifestation. A malignancy screen revealed an underlying nasopharyngeal carcinoma. (J Am Acad Dermatol 2003;48:S41-2.)
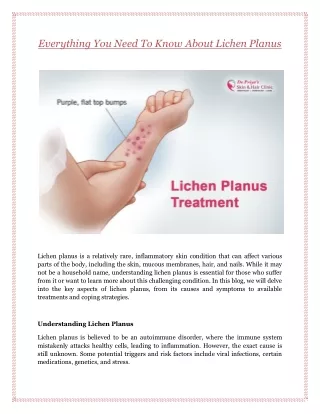
Lichen Planus • A disease of the skin, nails, hair follicles and mucous membranes. • Mnemonic the 5 P’s • Wickham’s Striae, flat topped papules • Pruritis is paroxysmal, rubbing > scratching • Flexor wrists, trunk, medial thighs, shins, dorsal hands, glans penis
Plentiful Purple Pruritic Polygonal Papules