Download
1 / 30
300 likes | 451 Views
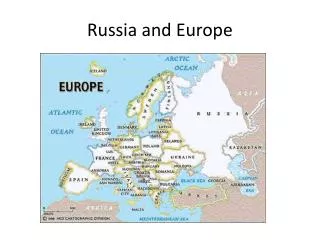
Social science of HIV and hepatitis C in Russia and southeastern Europe. Sergii Dvoriak M.D., Ph.D Ukrainian Institute on Public Health Policy, Kyiv, Ukraine. Symposium “Social and Structural Determinants of the HIV Epidemic in Eastern Europe and Central Asia”

E N D
Social science of HIV and hepatitis C in Russia and southeastern Europe SergiiDvoriakM.D., Ph.D Ukrainian Institute on Public Health Policy, Kyiv, Ukraine Symposium “Social and Structural Determinants of the HIV Epidemic in Eastern Europe and Central Asia” IAS 2013 7th IAS Conference on HIV Pathogenesis, treatment and Prevention 30 June – 03 July 2013 – Kuala Lumpur, Malaysia
UNAIDS, Global Report, 2011 FACT SHEET • Eastern Europe and Central AsiaA steep regional increase in new HIV infections and AIDS-related deaths • In EE&CA, the number of people living with HIV almost tripled between 2000 and 2009. An estimated 1.4 million [1.3 million–1.6 million] people were living with HIV in 2009 compared to 530 000 [470 000–620 000] in 2000. • AIDS-related deaths continue to rise in the region: an estimated 76 000 [60 000–95 000] people died from AIDS-related causes in 2009 compared to 18 000 [14 000–23 000] in 2001, a four-fold increase. • The Russian Federation and Ukraine together account for nearly 90% of newly reported HIV infections. • Ukraine has the highest adult HIV prevalence in all of Europe and Central Asia, at 1.1% [1.0%–1.3%]. Annual HIV diagnoses in Ukraine have more than doubled since 2001. • Between 2000 and 2009, the HIV incidence rate increased by more than 25% in five countries in the region: Armenia, Georgia, Kazakhstan, Kyrgyzstan and Tajikistan.
Social Determinants of Health Complex and overlapping community, social, economic, and environmental factors that influence an individual’s and a collective community’s risk for health inequities.
Structural factors on HIV-Epidemic • Health care and • Social welfare systems • Disease-specific public health response • Treating of vulnerable groups (PWID, Sex workers, prison populations etc.) • Evidence-based drug policy
Barriers • Unequal distribution of wealth and power; • Classism • Racism • Sexism • Homophobia • Transphobia • Narcophobia
Predisposition to DA Poverty Addiction + Risky Bhv Incarceration Unemployment HIV, HCV, Mental Health problems
The HIV Epidemic in Ukraine In 1995, the WHO characterized Ukraine as a low prevalence country. By 1996, all 25 regional capitals in Ukraine reported HIV, primarily among drug injectors. In some cities, rates of HIV among IDUs rose from nearly zero in 1994 to more than 50% two years later. Today, Ukraine is the most HIV-affected country in Europe and Central Asia, with an estimated 260,000 infected between the ages of 15 - 49, or 1.13% of the population in this age range. Prevalence among PWID – 21.5%. (Bio-behavioral Survey, 2011)
Social reasons: The social and economic disintegration that followed the collapse of theSoviet Union in 1991. With the withdrawal of the Soviet Union in December 1991: • Police controls became ineffective, drugs more readily available, and corruption uncontrolled. • In the first 5 years following the demise of the Soviet Union, the magnitude of the illicit economy was estimated to have tripled, reaching more than 40% of the gross national product from 1994 through1995. • Locally produced opiates and amphetamines proliferated. Registered drug users increased from 30,000 to 63,000 between 1990 and 1996. • State-supported services, including health care, were reduced or eliminated. • Robert Booth at all. 2013. AIDS Behav
Registered drug users in Central Asia (UNODC World Drug Report, 2010)
Russia • 547,000 – registered addicts • 102.5 mln of age 15-64 • Estimated Prevalence 1.64% Total ~1.68 mln drug users
HIV transmissioninUkraine • Injection of drugs • From mother to child • Sexual • Undetermined Data of the Ukrainian AIDS Center
Mode of Transmission Attributed to HIV Cases by Gender in Ukraine, 2005-2011
Monitoring of Epidemic Trends • The main indicator– HIV prevalence among high-risk groups • Example – HIV prevalence among IDUs using drugs at least 2 years • 2005г. – 23,8% • 2006г. – 20,2% • 2007г. – 18,9%
HIV prevalence among recent IDUs and IDU coverage by prevention programs, 2004-2011 • HIV Prevalence among recent IDUs (injecting for less than 3 years) was used as proxy incidence. • Median value for 8 cities: Donetsk, Lutsk, Odessa, Poltava, Simferopol, Summy, Kharkov, Kherson. • Prevention program coverage at last 12 month • With increasing coverage over the last 6 years, HIV incidence has been declining significantly: from 29.9% percent in 2004 to 5.5% in 2011 Coverage
Prevalence of Hepatitis C among People who Inject Drugs* *Cumulative information on infections over the last decades. Incidence of hepatitis C infections is unavailable in most countries.
STOP HARM REDUCTION! • Needle / syringes exchange programs stimulate a tolerance toward patients with drug abuse and violators of Russian federation’ legislation. Russian Minister of Health (2010)
“In honor of Hitler it was namedAdolphine and later Dolophine”. • “In the majority of nations methadone was completely prohibited. Any supply of this compound is stored and safely put away completely in the West”. • “Methadone was used as a detonator in conducting so called ‘colored’ revolutions. It was established with the breakup of Yugoslavia: there was a factory made for the production of methadone and it was distributed for free, until civil unrest. Then the factory was closed and thousands of drug users began to vandalize and destroy everything in their way”. • “RossiyskayaGazeta” About methadone
Russian Authorities are categorically against OST • “EC countries make a pressure to us for implementation of OST. They want we do treat drug addicts by other drugs”. • FDCS will not allow to stick Russia methadone therapy. • “The USA and some European countries support us”.
Study of Structural Barriers to HIV Prevention and Treatment Among Drug Injectors in Odessa, Ukraine (2010). • Legal and economy collapse leaded to increasing risky behavior. • The epidemic is largely sustained by the lack of government resources devoted to the problem, the continued risky drug using practices of injection and, • perhaps most importantly • by the risk environment • surrounding drug users. • Collaboration and especially financial support of government to NGOs is very poor.
Opinions of Most Effective Strategies for Treating Addiction (N=239)
CONCLUSIONS • Many social barriers in FSU countries continue to support the epidemics (HIV & HCV). • Joint efforts needed to change drug policy, drug treatment with HIV.HCV prevention; and eliminate stigma from PWID. • Drug policy and treatment/prevention approaches have to be based on scientific evidence. • Public health issues must be the priority
Contacts: dvoryak@uiphp.org.ua www.uiphp.org.ua Thank you for your attention.