Download
1 / 34
340 likes | 390 Views
Explore the key distinctions between root cause analysis and shallow cause analysis in improving performance and solving problems effectively. Learn the essential elements and tools for conducting analytical investigations.

E N D
Reliability Center, Inc. Presents…
rL Solutions i-Presentation Series Root Cause Analysis Versus Shallow Cause Analysis: What’s the Difference? Robert J. Latino EVP – Reliability Center, Inc.
RCI Background • Established in 1972 as Corporate R&D Reliability Center for Allied Chemical Corporation (now Honeywell) • Established Charter to Conduct Research and Develop in the Fields of Equipment, Process and Human Reliability • As an Independent Company in 1985, Able to Spread Reliability Concept and Methods to All Industry • Researched Healthcare Culture and Market with Fay Rozovsky of The Rosovsky Group in 1997 and Revised Methodologies & Software Accordingly • Experts in Critical Thinking Framework as opposed to content within given industries
Recent Publications • Root Cause Analysis: Improving Performance for Bottom-Line Results, 1999, 2002 and 2006, Robert J. Latino, Taylor & Francis • The Handbook of Patient Safety Compliance, 2005, Fay Rozovsky and Dr. Jim Woods, Jossey Bass [contributing author] • Error Reduction in Healthcare, 1999, Patrice Spath Editor, Jossey Bass [contributing author] • Taking Risky Business Out of the MRI Suite, Materials Management in Healthcare Magazine, 2006, Robert J. Latino, Fay Rozovsky and Tobias Gilk • Optimizing FMEA and RCA Efforts in Healthcare, ASHRM Journal, 2004, Volume 24, No. 3, pages 21 – 28 • Root Cause Analysis Versus Shallow Cause Analysis: What’s the Difference?”,Speaker, ASHRM 2005 National Conference • Intelligence and Security Informatics International Conference Proceedings, The Root Causes of Terrorism, May 2005, Department of Homeland Security (DHS)
Here We Go! 1. Analytical Process Review 2. Analytical Tools Review 3. A Case Study: Contrasting the Difference Hit any key to begin at your own pace.
Insanity is when we do the same thing over and over again and expect a different result. - Albert Einstein
Is This Insane? (A brief movie, 7 slides – hit any key to resume.
Brainstorming: A technique teams use to generate ideas on a particular subject. Each person in the team is asked to think creatively and write down as many ideas as possible. The ideas are not discussed or reviewed until after the brainstorming session. (ASQ) • Problem Solving: The act of defining a problem; determining the cause of the problem; identifying, prioritizing and selecting alternatives for a solution; and implementing a solution. (ASQ) • Trouble Shooting: To identify the source of a problem and apply a solution to "fix” it. (http://www.fairfield.k12.ct.us/develop/cdevelop02/glossary.htm) – Synonyms: Trial-And-Error and “Band-Aid Fixes”. • Root Cause Analysis: A method used to identify and confirm the causes of performance problems or adverse trends and identify the associated corrective actions needed to prevent recurrence of the causes. Root Cause Analysis (RCA) techniques apply investigative methods to unravel complex situations to determine root causes of performance problems, identify associated causal factors, check for generic implications of an event, determine if an event is recurrent, and to recommend corrective actions. (www.alwaysimproving.com)
The Essential Elements Of RCA • Identification of the Real Problem to be Analyzed in the First Place • Identification of the Cause-And-EffectRelationships that Combined to Cause the Undesirable Outcome • Disciplined Data Collection and Preservation of Evidence to Support Cause-And-Effect Relationships • Identification of All Physical, Human and Latent Root Causes Associated with Undesirable Outcome • Development of Corrective Actions/Countermeasures to Prevent Same and Similar Problems in the Future • Effective Communication to Others in the Organization of Lessons Learned from Conclusions If any one of these essential elements are missing, then we are not doing true “RCA”.
4 1 2 3 Why? How Can? Why? How Can? Why? How Can? Why? How Can? 5 Why? Common Analysis Process Tools LOGIC TREE 5-WHYS FISHBONE
1 2 3 4 Why? Why? Why? Why? 5 Why? The 5 - Whys 5-WHYS • Uses Limited Cause-And-Effect • Modes Are Dependent Upon Each Other • Uses Linear Path by Asking WHY? • Promotes Use of Opinion as Fact • Promotes Belief That Only One (1) Root Cause Exists
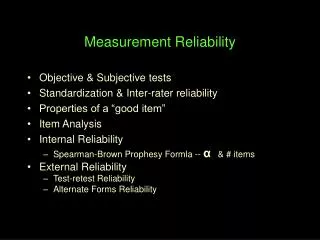
The Ishikawa Fishbone Diagram FISHBONE • Does NOT Use Cause-And-Effect • Modes Are NOT Dependent Upon Each Other • Uses Brainstorming Primarily • Allows Use of Opinion as Fact • Promotes Belief That All Causes Are Within Categories Used • Commonly Used Categories (Fish Bones) • Methods, Machines, Materials & Manpower (4-M’s) • Place, Procedure, People & Policies (4-P’s) • Surroundings, Suppliers, Systems & Skills (4-S’s)
Essential Elements of RCA Preserving Event Data Ordering the Analysis Team Analyzing Event Data Communicating Findings & Recommendations Tracking For Bottom Line Results
How Could? How Could? How Could? How Could? Why? Logic Tree LOGIC TREE EVENT • Uses Cause-And-Effect • Modes Are Dependent Upon Each Other • Seeks All Possibilities By Asking HOW CAN? • Uses Evidence to Prove All Hypotheses • Identifies Decision Making Errors and Systems Flaws MODES
Consequence X X Response Events vs. Modes Accident/Incident Did the response to the accident/incident make the consequences worse?
{ Consequences HOW’s Actions { Component Causes (Physical) WHY’s Decision Roots (Human) Intent Deficiencies in Organizational Systems (Latent) The “Root” System
Physical Decision Roots (Human) Mis- Construction (Mis-Perception) Stress and Workload (Tunnel Vision) Coordination Failures (Goals & Priorities) New Technology (Automation) Latent Plan Continuation (Cues) Normalization Of Deviance (Safety) Failures To Adapt (Procedures) Breach Of Defenses (Swiss Cheese) Some Human Factors Affecting Decision Making Source: The Field Guide to Human Error Investigations – Sydney Dekker, Ashgate, 2002.
What Do You See?The Mind is a Mysterious Thing A bird in the the hand is worth two in the bush Perceptions are mental models developed in the brain to interpret incoming information the way it SHOULD BE versus the way that it IS.
L A H T P U E H M N Y A T S N I C A L Remember The Swiss Cheese Model? James Reasons, Human Error, 1990 Defenses (Barriers)
Contrast to A Detective’s Role RCA ANALYSTS DETECTIVES “Police Scene” Top Box Crime Event Facts Failure Modes Hypotheses/ Verification Leads/ Evidence Forensics (How’s) Physical Roots (Consequences) Human Roots (Actions) Opportunity Latent Roots (Intent) Motive (Why’s)
Software Based RCA: Effectiveness vs. Efficiency vs. Strength of Evidence Hi Hi Disciplined RCA Accuracy (Effectiveness) Strength of Evidence Problem Solving Brainstorming Lo Lo Trouble shooting Months Hours Time (Efficiency)
1 2 3 4 Why? How Can? Why? How Can? Why? How Can? Why? How Can? 5 Why? Breadth and Depth Check Breadth Depth LOGIC TREE 5-WHYS FISHBONE
A Case Study: Endobronchial Fire R.P.: A 65 year old man was admitted with hemoptysis in October 2002. He underwent right upper lobectomy on December 14, 1999. His final diagnosis was adenocarcinoma (T1NoMo). He received radiotherapy and chemotherapy for recurrent malignancy in August of 2002. During this admission he was found to have bleeding from an obstructing tumor of the right main stem bronchus. Laser bronchoscopy was performed on October 7, 2002. During the procedure, endobronchial fire occurred. This was treated with prompt removal of bronchoscope and endotracheal tube. The patient was reintubated and irrigated with Normal Saline. The patient survived this event, but died in July of 2003 from metastatic lung cancer.
Endotracheal Fire During Bronchoscopy Fire Initiated in Right Bronchus Fuel Source Present in Right Bronchus Nitrogen Used to Ventilate Chamber Too Much Nitrogen Introduced Sample 5-Why Why? Why? Why? Why? Why?
Methods Machines Bronchoscopy Procedure Issue Faulty Bronchoscope Source Anesthetic Procedure Issue Fiber Optic Assembly Issue Scheduling/Timing Issue Manufacturer Overload Fire in Endotrachial Tube During Bronchoscopy Nitrogen Issue Anesthesiologist Error Inexperienced Foreign Debris/ Contamination Surgeon Error Fatigued Materials Manpower Sample Fishbone (4-M’s)
HR Sample Logic Tree E = Effect E OR/Patient Fire - Sentinel Event C = Cause C Endotrachial Fire During Yag Laser Bronchoscopy E Fire Occurred Prior to Procedure Fire Occurred During Procedure Fire Occurred After Procedure C E Fire Initiated inside the Right Bronchus Fire Initiated Outside the Right Bronchus C Presence of Sufficient Oxygen Presence of Sufficient Fuel Presence of Sufficient Ignition Source Sufficient Fuel Source Within Patient Sufficient Fuel Source Introduced Into Patient Sufficient Fuel Source On OR Staff Sufficient Fuel Source within Atmosphere Smoldering Tumor Generating Smoke Plume Bronchoscope Source Laser And Fiber Optic Assembly Damaged Suff. Additional Gases Intro’d And Exposed To Laser ET Tube Ignited Foreign Debris B A
LR LR LR LR HR PR HR Sample Logic Tree (Cont’d) A B Laser Mis-Fired In Bronchoscopy Tube Oper. Channel Contaminated Operating Channel Mismanagement of Anesthetic Gas Contaminated During Cleaning Process Chemical Contamination QC Issue - Failure to Detect Contamination Decision to Clean Equipment Using Flammable Agent QC Inspection in Place and Not Followed No QC Inspection in Place QC Inspection in Place Less Than Adequate Decision Not in Accordance With Procedure Decision in Accordance with Procedure Current Procedure Inappropriate Purchasing Pressures (Finance vs. Functionality) No Review Process of Current Proc. When Vendors Change
Root Causes Identified 5-Whys Fishbone PROACT RCA Too Much Nitrogen Introduced X X X Anesthetic Procedure Issue X Evidence proves this not to be true Fiber Optic Assembly Issue X Evidence proves this not to be true Anesthesiologist Error X X Contaminated Operating Channel of Brochoscope Source X Contamination During Cleaning Process Using Flammable Agent X Purchasing Pressures to Reduce Cost X No QC Review Process in Place When Evaluating New Vendor’s Offerings X Failure to Detect Contamination Prior to OR Use X No QC Inspection of Cleaned Instruments Prior to Use in OR X Sufficient Additional Gases Introduced and Exposed to Laser X Mismanagement of Anesthetic Gases X Filtering the Results?
Conclusion • We should be doing analyses to the breadth and depth of RCA when warranted simply because it is the right thing to do (chronic versus sporadic)! • If we are doing true RCA, compliance will be a by-product. If it is not, there is something very wrong with the regulations/ guidelines. • Our RCA efforts should be directly correlated to patient safety/impact on the patient. • We should thoroughly understand when it is appropriate to use RCA and when it is appropriate to use shallow cause approaches. The rigor of RCA is not appropriate for every situation that arises. • Using “shallow cause” approaches when “root cause” approaches are warranted, will likely result in the missing of key systemic root causes. This will increase the risk of recurrence. Are we using the appropriate tools for the appropriate situations?
Thank you for your time and interest!QUESTIONS? For more Information on PROACT, LEAP, FMEA, or Root Cause Analysis in Healthcare contact Gary Bonner at Reliability Center Inc. (RCI) by calling 804.458.0645 or sending an e-mail to gbonner@reliability.com www.proactforhealthcare.com www.reliability.com For more information on the rL Solutions product suite, or to learn more about how we have integrated PROACT into our solutions please contact Mike Smith at rL Solutions by calling (416) 410-8456 x 287 or sending an e-mail to msmith@rl-solutions.com www.rl-solutions.com