Download
1 / 94
1.06k likes | 2.46k Views
The red eye for the primary care provider. Donald J. Costello, O.D. Emergent referrals. If patient needs to be seen today, call or text me If urgent (48 hours) or unsure, give contact info to Julia and we will triage If non-urgent contact front desk Mobile: 504-237-3875

E N D
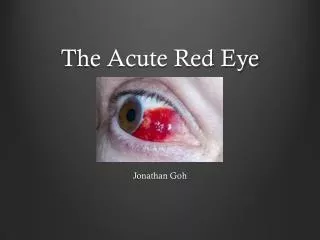
The red eye for the primary care provider Donald J. Costello, O.D.
Emergent referrals • If patient needs to be seen today, call or text me • If urgent (48 hours) or unsure, give contact info to Julia and we will triage • If non-urgent contact front desk • Mobile: 504-237-3875 • Email:costello@stthomaschc.org • MJ Front Desk: 504-359-6807
ConjuntivitisAka “Pink eye” • Definition: Inflammation or infection of the conjunctiva
Conjuntiva • Definition: The thin transparent layer of tissue that lines the inner surface of the eyelid and covers the white part of the eye
Diagnosis • Patient History and Symptoms • External Exam • Slit Lamp Examination or Burton Lamp Exam • Other Testing: Labs, cultures, scrapings, biopsy, imaging
TOOLS FOR THE PRIMARY CARE PROVIDER • History/Symptoms • Preauricularadenopathy • Signs: Papillary vs. Follicular Reaction • Type of Discharge • Corneal involvement (Burton Lamp)
Examination techniques Burton Lamp Slit Lamp
Examination techniques Sodium Fluorescein Corneal Staining
Differential Diagnosis“Doc, I think I have a pink eye” • Bacterial • Adenoviral (pink eye) • Herpetic Viral • Other Viral • Fungal • Chlamydial • Spirochete • Nematode • Amoeba • Inflammation • Allergic • Dry Eyes • Contact Lens Related • Radiation • Exposure • Thygeson’s
Differential Diagnosiscontinued • SLK • Neuroparalytic • Pterygium • Aerosol/Chemical • Degenerations • Ulcers • Ligneous • Steven’s Johnson’s Syndrome • Ocular Rosacea • Blepharitis • CicatricialPemphigoid • Recurrent Corneal Erosion • Keratoconus with Hydrops • Acute Angle Closure Glaucoma • Foreign Body
Differential Diagnosiscontinued • Post Surgical • Trichiasis • Distichiasis • Episcleritis • Scleritis • Uveitis • Dellen • Phlyctenule • Giant Papillary Conjunctivitis • Parinaud’sOculoglandular Conjunctivitis • Mucous Fishing Syndrome • Floppy Eyelid Syndrome • Medicamentosa • Retention Cyst • Neoplastic…..and MORE
Conjuntivitis/Red Eye • These All present as a RED EYE
Categorize Red eye • Acute vs. Chronic • Infectious vs Non-infectious • Cause of Infection/Inflammation • Adults vs. Children • Unilateral vs. Bilateral • Signs on Slit Lamp • Patient Symptoms
Acute red eye • Duration less than 4 weeks • If chronic and unilateral then best to refer out • If chronic and bilateral, try lubrication and lid scrubs and if no improvement refer out
Causes • Infectious (bacterial, viral, fungal, chlamydial, amoeba) • Allergic Inflammation (histamine) • Inflammation (not histamine related) • Dry Eyes and Blepharitis • Toxic • Other
Infectious cause • Bacterial • Viral Non-Herpetic (eg. Adenoviral) • Viral Herpetic • Fungal • Chlamydial/Gonococcal • Amoeba/protozoan
Inflammatory cause • Allergic: Type I and Type IV allergic rxn • Episcleritis/scleritis/iritis • Dry eyes/blepharitis
Toxic and Other Causes • Medicamentosa • Subconjunctival hemorrhage • Foreign body • Keratoconus with acute hydrops • Acute angle closure glaucoma • Contact lens related (infectious and inflammatory)
Bacterial ConjuctivitisSigns/symptoms/treatment • Conjunctival Injection • Purulent green/yellow discharge • Papillary rxn • Minimal to no preauricular node • Chemosis • Uncommon in adults, common in children • Treatment: Fluoroquinolone (Vigamox), Polytrim
Bacterial KeratitisSigns/Symtoms/treatment • Vision Threatening • Little to no discharge • Photophobia, pain, conjunctival injection • Contact Lens wear common cause • Burton Lamp/Slit Lamp to diagnose • Treatment: Fluoroquinolone every 30 mins for 6 hours, then hourly
Bacterial conjunctivitis vs keratitis Bacterial Conjunctivitis Bacterial Keratitis
What about mrsa? • Any bacterial conjunctivitis unresponsive to treatment • Culture • Treat with Besivance, Fortified Vancomycin, Imipenem • ARMOR Study: Antibiotic Resistance Monitoring in Ocular MicRorganisms
Viral Conjunctivitis/Non herpeticSigns/symptoms • Contagious (5-14 days) • Common • AKA “Pink Eye” • Follicular rxn • Preauricular node • Watery discharge with lids crusted closed in AM • Hyperemia • Discomfort/ Pain if cornea involved • May be associated with respiratory infection • May have petechialsubconj. Hemes • Self limiting • Often Adenoviral (31 serotypes/10 cause conj)
Diagnosis of adenoviral conjuntivitis RPS AdenoPlus detector Plus Cost: $ 40.25/patient 96% Specificity 90% Sensitivity Results in 10 minutes Best if used within 10 days of developing red eye
Viral Conj/Types • Epidemic Keratoconjunctivitis (EKC) • Adenovirus types 8+19 • Not associated with respiratory symptoms • Bilateral 2/3 of cases • Clinical course of 7-14 days • Corneal Infiltrates 80 % of cases/ Pain, decrease VA • Contagious up to 2 wks
EKC Follicular Conjunctivitis
EKC Pseudomembrane
EKC Corneal Sub-epithelial Infiltrates
Treatment EKc • Palliative: preservative free artificial tears every 2 hours for comfort (Refresh Plus/Systane Free) • Topical Steroids or steroid/antibiotic combination drops (Tobradex, Zylet, Maxitrol) 4 times per day for five days • Topical steroids give comfort and preserves vision from sub-epithelial infiltrates
Viral Conj/types • Pharyngoconjunctival Fever (PCF) • Adenovirus type 3+7 • Pharyngitis, fever • Unilateral • Clinical course 5-14 days • Contagious 10-12 days • Corneal infiltrates mild
Viral Conj/Types • Acute Hemorrhagic Viral Conjunctivitis • Many micro subconjunctival hemorrhages • Enterovirus 70 • Resolves in 7 days
Differential Diagnosis (Acute Hemorrhagic Conj) Sub Conjunctival Hemorrhage No discharge No discomfort Usually unilateral Remainder of conj is white No follicles
Treatment of non herpetic Viral Conjunctivits • Palliative: Preservative free artificial tears every 2 hours • Topical steroid drops or ab/steroid drops four times per day: More effective later in course of the conjunctivitis • Other Treatments: Betadine (povidone-iodine) 1.25% for 1 week, or 5% single dose • Ganciclovir gel • Cidofovir: effective but causes punctal stenosis
Bacterial vs viral conjuntivitis • Bacterial • Papillary rxn • Unilateral often • Green/yellow discharge • Uncommon • Viral • Follicular rxn • Often bilateral • Watery discharge • Respiratory Infection • Preauricular node • Contagious (family may have it) • Common
Papillary ConjunCtivitis Papillae are vascular structures invaded by lymph cells Vessel runs up center of papilla Common in allergic conjunctivitis and sometimes bacterial
Follicular ConjunCtivitis Minute lymph nodes Vessels run in the periphery of the follicle Not present until 2-3 months of age Common in viral, chlamydial, and toxic conjunctivitis
Molluscumcontagiosum Nodules with umbilicatedcenters Follicular Conjunctivitis Watery Discharge Common in children If left untreated can leak to spk, sei’s and corneal vasculariztion Treatment: Removal by cauterization, cryotherapy, excision Pox virus Diff. Dx: Sebaceous cyst, verruca, Chalazion
Herpetic KeratoconjunCtivitis • The masquerader • Primary Ocular Herpes • Recurrent Herpes Simplex Keratitits (HSK) • Herpes Zoster Ophthalmicus (HZO)
Primary Ocular Herpes • Acute Follicular Conjunctivitis often with preauricularadenopathy with or without a lid lesion • Self limiting • Cornea may have superficial punctate keratitis • Virus develops a latent infection in the trigeminal ganglion
Recurrent Herpes Simplex Keratitis (HSK) Corneal epithelium infected (dendrite) Stromal Keratitis/Disciform Keratitis Any layer of eye can become infected (iritis/retinitis) Usually unilateral and recurrence on same side (dermatome) Decreased corneal sensitivity Common More than 90%humans carry latent virus May have history of lip sores