Download
1 / 25
450 likes | 1.6k Views
Ventricular septal defect . Moderator – Dr Bhalla Presentor – Dr Priya. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Harneet 8m male child Resident of Ludhiana Informant : mother. Chief complaints. Difficulty in feeding × 7 m Increased respiratory rate × 7m. HOPI :.

E N D
Ventricular septal defect Moderator – Dr Bhalla Presentor – Dr Priya www.anaesthesia.co.in anaesthesia.co.in@gmail.com
Harneet • 8m male child • Resident of Ludhiana • Informant : mother
Chief complaints • Difficulty in feeding × 7 m • Increased respiratory rate × 7m
HOPI : • H /O sweating while feeding , frequent interruption while feeding • H/O fast breathing with chest retractions • H/O visible cardiac pulsation • H/O poor weight gain
No H/O bluish discolouration while crying • No H/O abdominal distention • ↓urine output • swelling of face and feet • No H/O fever with spots over body
Past history : • No history of any other illness in past • Family history : first child , no similar complaints • Antenatal history : • Regular follow up • No intake of drugs , no H/O fever with rash • USG normal
Birth history : full term vaginal delivery at hospital • Cried immediately after birth • Developmental history : • Can sit without support and hold head • Immunization history : • Adequately immunized for age
Treatment history : • Furosemide + spironolactone and digoxin
General physical examination : • Conscious lying on bed • Pallor – absent • No cyanosis ,ikterus , clubbing or edema • VITALS: • PR :120 /min regular rhythm ,normal volume ,no delay • BP: 86/ 50 mm hg right arm supine • RR : 48/min subcostal retractions present
Temp : afebrile to touch • Height : 64 cm • Weight : 6.2kg • Anterior fontanalle : not depressed • Venous access : adequate • No other visible malformations
Systemic Examination :- • Cardiovascular system : • Inspection :- precordial bulge - present visible pulsation + no scar mark abnormality of skeletal structure. • Palpation :- Apex beat – left 5th ICS in MCL palpable thrill. parasternal lift.
Auscultation :- S1 & S2 audible S2 accentuated & split over pulmonary area. Pan-systolic murmur at apex & LLSB.
Respiratory system : • Inspection : no visible chest wall deformity • No visible pulsation seen • Auscultation: B/L vesicular air sounds +, no added sounds Central nervous system :- • conscious, apathetic • no sensory or motor deficit • reflexes normal.
Provisional diagnosis :- Acyanotic congenital heart disease with left to right shunt without CHF or infective endocarditis
Investigations: • Hb – 11.2 • TLC – 9600 • Na /K – 146/ 4.6 • CXR - cardiomegaly , ↑ pulmonary vascularity • Echo : LA + LV enlarged , RA/ RV normal , 8 mm mid muscular VSD , mild MR
Prevalence Congenital Incidence of CHD :8 / 1000 live birth • Cyanotic: 22% • Acyanotic: 68% • VSD 25% • ASD 6% • PDA 6% • PS 5% • AS 5%
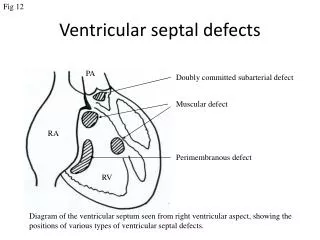
VSD • Most common CHD • 2.6 to 5.7 /1000 live birth • 10 % of adult CHD • TYPES :- • Subpulmonary (5-7 % )- with AV insufficiency • Perimembranous (80 %)-with tricuspid valve abnormality • A-V canal (5-8%) • Muscular (5 -20 % )- multiple defect • Restrictive , non- restrictive • Small, medium, large (in relation to aortic root )
Syndrome associated with VSD • Extra cardiac malformation in 20-45 % - Trisomy 21,18,13 - CHARGE syndrome - Fetal hydantion syndrome - Fetal alcohol syndrome - Fetal valproate syndrome - Apert syndrome
Severity of VSD :– - loud P2, parasternal lift/heave - duration of murmur - diastolic murmur at mitral area - features of CCF
LARGE L- R SHUNT ↑ PVR ↑ LA SIZE ↑LA PRESSURE INTERSTITIAL AND ALVEOLAR EDEMA ↑ PA FLOW ↑PA PRESSURE ENLARGEMENT OF VESSELS BRONCHIAL HYPERTROPHY AIRWAY OBSTRUCTION ↑ AIRWAY RESISTANCE ↓ PULMONARY COMPLIANCE INCREASED WORK OF BREATHING GAS TRAPPING, ATELECTASIS, INFECTION
NATURAL HISTORY • Spontaneous closure of defects less than 5mm before 5 yrs of age (40-50%). • Natural course depends on – size, change in PVR, age • Large defects – CHF in infancy (2-6 wks), when PVR falls • Tachypnea, Distress, Sweating while feeding, Failure to thrive • CHF- apathetic, no movement, weak cry, diaphoretic, hepatomegaly • Indications for surgical closure- >6.5 mm, Qp:Qs ratio >2