Download
1 / 25
340 likes | 1.38k Views
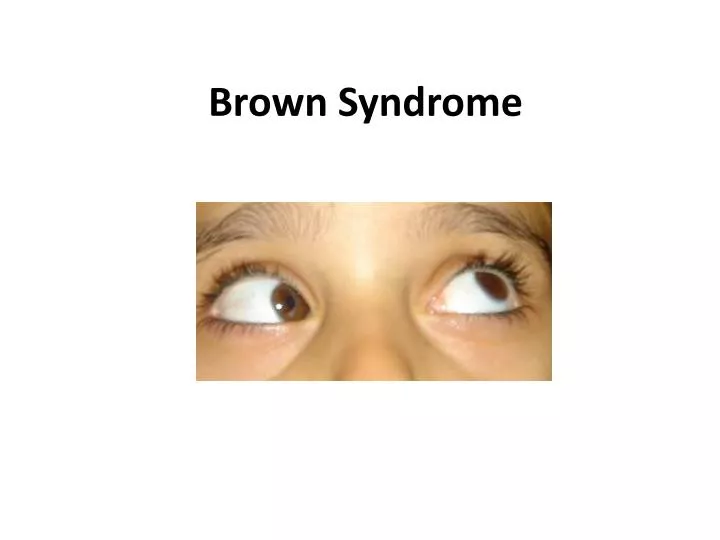
Brown Syndrome. Brown syndrome is found in 10% to 24% of patients with vertical muscle paresis. occur once in every 430 to 450 cases of strabismus. may be bilateral in approximately 10% of case. Brown syndrome was described by Harold W. Brown in 1949 as the superior oblique tendon

E N D
Brown syndrome is found in 10% to 24% of patients with vertical muscle paresis. . occur once in every 430 to 450 cases of strabismus. . may be bilateral in approximately 10% of case
Brown syndrome was described by Harold W. Brown in 1949 as the superior oblique tendon sheath syndrome. MECHANISM Shortening of the anterior sheath of the superior oblique tendon. Restriction of the superior oblique tendon at the trochlear pulley • this theoryabandoned congenitally inelastic or short tendon Abnormal tendon-trochlear complex
Brown Syndrome Restriction of the superior oblique tendon at the trochlear pulley
FINDING • 1. Deficient elevation in adduction • 2. Less elevation deficiency in midline . • 3. Minimal or no elevation deficiency in the abducted position • 4. Minimal or no SO overaction.. • 5. V pattern with divergence in upgaze • 6. Restricted forced ductions
OTHER FINDINGS • 1. Downshoot or hypotropia in adduction • 2. Widening of the palpebral fissure on adduction • 3. Anomalous head posture • 4. Hypotropia in the primary position
DIFFERENTIAL DIAGNOSIS • 1-I O PALSY • 2-DOUBLE ELEVATOR PALSY • 3- CONGENITAL FIBROSIS SYNDROM • 4-BLOW OUT FX • 5-THYROID OPHTHALMOPATY • 5-ADHERENCE SYNDROM
Brownsyndrome Resolution of congenital Brown syndrome is unusual but possible Congenital Acquired form Trauma in the region of the trochlea Systemic inflammatory Iatrogenic Brown syndrome intermittent Brown syndrome, which may resolve spontaneously.
Comparison of Inferior Oblique Muscle Palsy With Brown Syndrome Deficient elevation in adduction that improves in abduction but often not completely In adduction, the palpebral fissure widens and a downshoot of the involved eye is often seen; it can be distinguished from superior oblique muscle overaction because downshoot in the latter condition occurs less abruptly as adduction is increased.
Brown syndrome OS Divergence in upgaze Down shoot in attempted elevation in adduction? Down shoot in attempted elev. in adduct. (different than IO palsy)
Brown syndrome chin-up head posture and sometimes by a face turn away from the affected eye in sever cases
An unequivocally positive forced duction test demonstrating restricted passive elevation in adduction is essential for the diagnosis of Brown syndrome. Retropulsion of the globe during this determination stretches the superior oblique tendon and accentuates the restriction. When inferior rectus muscle fibrosis or inferior orbital blowout fracture (the principal entities to be differentiated) produces a restrictive elevation deficiency, the limitation to passive elevation is accentuated by forceps-induced proptosis of the eye rather than by retropulsion.
Management 1.Observation :alone in about two thirds of all Brown syndrome cases 2.rheumatoid arthritis or other systemic inflammatory diseases Systemic treatment 3.Corticosteroids injected near the trochlea 4.Sinusitis has also led to Brown syndrome CT of the orbits and paranasal sinuses
Surgical treatment is indicated for the most severe cases Primary position hypotropia Anomalous head posture Iatrogenic superior oblique muscle palsy may occur postoperatively. 44%-82% sheathectomy has been abandoned in favor of ipsilateral superior oblique tenotomy
Brown Syndrome SO tenotomy SR SR LR RM MR LR IR IR IO IO
Superior oblique muscle palsy Reduced: By careful preservation of the intermuscular septum during tenotomy. This modification often produces an early under correction that gradually improves with time
Perform simultaneous ipsilateral inferior oblique muscle weakening. guarded tenotomy using an inert spacer sewn to the cut ends of the superior oblique tendon Controlling the gap between the cut ends with an adjustable suture These procedures eliminate the need for simultaneous inferior oblique muscle weakening but sometimes result in a downgaze restriction due to adhesions to the nasal border of the superior rectus muscle. Care must be taken to avoid contact of the spacer to nearby structures by preserving the intermuscular septum
In 1991, Wright described a superior oblique expander procedure for browns syndrome and superior oblique overaction with good results. Originally, this procedure has been performed with silicone band expander. .