Download
1 / 1
10 likes | 232 Views
Changes in Vision, Balance, Gait, and Dizziness with Balance-Based Torso-Weighting: A Case Report on a Woman with MS Cynthia Gibson-Horn, PT Laurie Chaikin, OD, OTR/L, FCOVD. Background

E N D
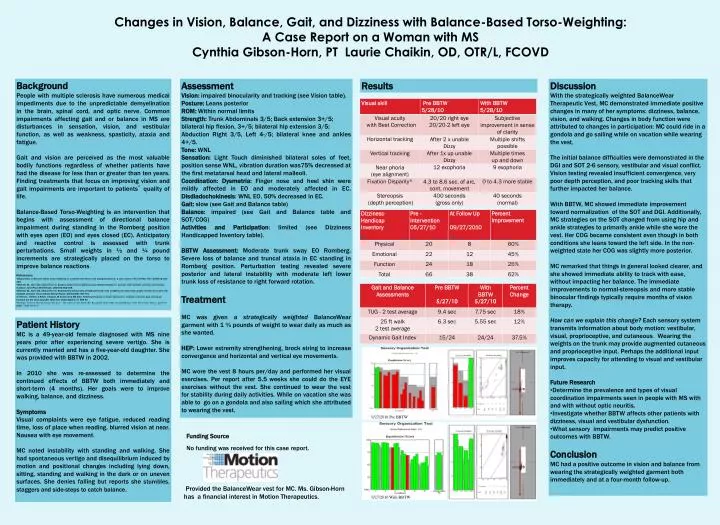
Changes in Vision, Balance, Gait, and Dizziness with Balance-Based Torso-Weighting: A Case Report on a Woman with MS Cynthia Gibson-Horn, PT Laurie Chaikin, OD, OTR/L, FCOVD • Background • People with multiple sclerosis have numerous medical impediments due to the unpredictable demyelination in the brain, spinal cord, and optic nerve. Common impairments affecting gait and or balance in MS are disturbances in sensation, vision, and vestibular function, as well as weakness, spasticity, ataxia and fatigue. • Gait and vision are perceived as the most valuable bodily functions regardless of whether patients have had the disease for less than or greater than ten years. Finding treatments that focus on improving vision and gait impairments are important to patients’ quality of life. • Balance-Based Torso-Weighting is an intervention that begins with assessment of directional balance impairment during standing in the Romberg position with eyes open (EO) and eyes closed (EC). Anticipatory and reactive control is assessed with trunk perturbations. Small weights in ½ and ¼ pound increments are strategically placed on the torso to improve balance reactions. • References • Gibson-Horn C. Balance-based torso-weighting in a patient with ataxia and multiple sclerosis: a case report. J Neurol Phys Ther. 2008;32:139-146. • Widener GL, Allen DD, Gibson-Horn C. Balance-based torso-weighting may enhance balance in persons with multiple sclerosis: preliminary evidence. Arch Phys Med Rehabil. 2009;90:602-609. • Widener GL, Allen DD, Gibson-Horn C. Randomized clinical trial of balance-based torso weighting for improving upright mobility in people with multiple sclerosis. Neurorehabil Neural Repair. 2009;23(8):784-791. • C Heesen, J Böhm, C Reich, J Kasper, M Goebel and SM Gold, Patient perception of bodily functions in multiple sclerosis: gait and visual function are the most valuable. Mult Scer 2008 Aug:14 (7): 988-91 • Multiple Sclerosis The Questions You have - The Answers You Need, By: Rosalind C Kalb, PhD, Second Edition, 2000, New York: Demos, pp37-39. ISBN: 1 888 799 43 9 Assessment Vision: impaired binocularity and tracking (see Vision table). Posture: Leans posterior ROM: Within normal limits Strength: Trunk Abdominals 3/5; Back extension 3+/5; bilateral hip flexion, 3+/5; bilateral hip extension 3/5; Abduction Right 3/5, Left 4-/5; bilateral knee and ankles 4+/5. Tone: WNL Sensation: Light Touch diminished bilateral soles of feet, position sense WNL, vibration duration was75% decreased at the first metatarsal head and lateral malleoli. Coordination: Dysmetria: Finger nose and heel shin were mildly affected in EO and moderately affected in EC. Disdiadochokinesis: WNL EO, 50% decreased in EC. Gait: slow (see Gait and Balance table) Balance: impaired (see Gait and Balance table and SOT/COG) Activities and Participation: limited (see Dizziness Handicapped Inventory table). BBTW Assessment: Moderate trunk sway EO Romberg. Severe loss of balance and truncal ataxia in EC standing in Romberg position. Perturbation testing revealed severe posterior and lateral instability with moderate left lower trunk loss of resistance to right forward rotation. Treatment MC was given a strategically weighted BalanceWear garment with 1 ¾ pounds of weight to wear daily as much as she wanted. HEP: Lower extremity strengthening, brock string to increase convergence and horizontal and vertical eye movements. MC wore the vest 8 hours per/day and performed her visual exercises. Per report after 5.5 weeks she could do the EYE exercises without the vest. She continued to wear the vest for stability during daily activities. While on vacation she was able to go on a gondola and also sailing which she attributed to wearing the vest. Results • Discussion • With the strategically weighted BalanceWear Therapeutic Vest, MC demonstrated immediate positive changes in many of her symptoms: dizziness, balance, vision, and walking. Changes in body function were attributed to changes in participation: MC could ride in a gondola and go sailing while on vacation while wearing the vest. • The initial balance difficulties were demonstrated in the DGI and SOT 2-6 sensory, vestibular and visual conflict. Vision testing revealed insufficient convergence, very poor depth perception, and poor tracking skills that further impacted her balance. • With BBTW, MC showed immediate improvement toward normalization of the SOT and DGI. Additionally, MC strategies on the SOT changed from using hip and ankle strategies to primarily ankle while she wore the vest. Her COG became consistent even though in both conditions she leans toward the left side. In the non- weighted state her COG was slightly more posterior. • MC remarked that things in general looked clearer, and she showed immediate ability to track with ease, without impacting her balance. The immediate improvements to normal-stereopsis and more stable binocular findings typically require months of vision therapy. • How can we explain this change? Each sensory system transmits information about body motion: vestibular, visual, proprioceptive, and cutaneous. Wearing the weights on the trunk may provide augmented cutaneous and proprioceptive input. Perhaps the additional input improves capacity for attending to visual and vestibular input. • Future Research • Determine the prevalence and types of visual coordination impairments seen in people with MS with and with without optic neuritis. • Investigate whether BBTW affects other patients with dizziness, visual and vestibular dysfunction. • What sensory impairments may predict positive outcomes with BBTW. • Conclusion • MC had a positive outcome in vision and balance from wearing the strategically weighted garment both immediately and at a four-month follow-up. Patient History MC is a 49-year-old female diagnosed with MS nine years prior after experiencing severe vertigo. She is currently married and has a five-year-old daughter. She was provided with BBTW in 2002. In 2010 she was re-assessed to determine the continued effects of BBTW both immediately and short-term (4 months). Her goals were to improve walking, balance, and dizziness. Symptoms Visual complaints were eye fatigue, reduced reading time, loss of place when reading, blurred vision at near. Nausea with eye movement. MC noted instability with standing and walking. She had spontaneous vertigo and disequilibrium induced by motion and positional changes including lying down, sitting, standing and walking in the dark or on uneven surfaces. She denies falling but reports she stumbles, staggers and side-steps to catch balance. 9/27/2010 Pre BBTW Funding Source No funding was received for this case report. Provided the BalanceWear vest for MC. Ms. Gibson-Horn has a financial interest in Motion Therapeutics. 9/27/2010 With BBTW