Download
1 / 17
170 likes | 338 Views
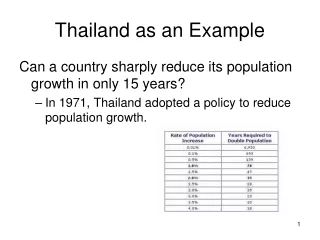
Selecting hospital records for injury surveillance: Australia as an example. James Harrison Research Centre for Injury Studies Adelaide, South Australia September 2006. Acknowledgements. Jesia Berry Geoffrey Henley Malinda Steenkamp Clare Bradley. Context.

E N D
Selecting hospital records for injury surveillance: Australia as an example James Harrison Research Centre for Injury Studies Adelaide, South Australia September 2006
Acknowledgements • Jesia Berry • Geoffrey Henley • Malinda Steenkamp • Clare Bradley
Context • The purpose is national injury surveillance • especially for primary prevention of injury in the general community • also interest in outcomes, costs, injury & other complications of care • Australia’s federal political system shapes the hospital system & its data • the 8 states & territories operate most of the hospitals • the Commonwealth raises and distributes most of the money • the public money is allocated by a system using Diagnosis Related Groups (DRGs) • Mixed public-private hospital system • acute care of serious injury is mostly in the public sector • About 350 thousand admitted injury cases / year • +/- a bit, depending on definition, selection criteria, etc. • (nearly) complete annual national unit-record files (for public and private hospitals) • each record = an episode of in-patient care (not a person or a case) • records include codes for Principal & Additional diagnoses & external causes • ICD-10-AM (Australian Modification) since 1998-99; new edition each 2 years
Purpose • How much (serious) injury occurs in Australia? • What are the injuries? • Diagnoses, body parts affected • How does injury occur? • External causes, etc • How is it distributed? • By person • age, sex, Indigenous status, etc. • By place • State/territory, remoteness, etc. • Over time • trends • What are its consequences? • Survival, hospital utilisation, rehabilitation, quality of life, economic costs, etc
Background • Usable national hospital data not available until early to mid 1990s • Improvement largely driven by change to DRG-based payment for public hospital services • Our early reports (late 1990s) • Much time spent learning about the data • Very cautious about claiming to be able to provide reliable information on trends and differences • This experience prompted development of a conceptual approach and plan • Technical review & documentation of current NHPA indicators and data sources (2002) • Our thinking was influenced by the Injury ICE • Commenced a program of development projects • Recent reports • 2001-02, 2003-04 (under review), 2004-05 (early stages of preparation) • More comprehensive and coherent • Each has similar structure, adding refinement and features in each edition • Largely restricted to data since late 1990s (Quality seems to be better; avoids complications of bridging ICD-9-CM to ICD-10-AM)
Case selection criteria • Issues considered in specifying criteria: • Period • Place/person • Condition • Counting incident cases once and only once • Minimising effect of variation in probability of detection of an incident case
Case selection criteria • Issues considered in specifying criteria: • Period • Place/person • Condition • Counting incident cases once and only once • Minimising effect of variation in probability of detection of an incident case
Case selection criteria • Issues considered in specifying criteria: • Period • Year of separation (~discharge). Ideally, period of injury. • Place/person • (Almost) all acute hospitals in Australia. Some numerator-denominator mismatch (inward & outward visitors, etc). • Condition • Counting incident cases once and only once • Using an approximate method; working on person-linkage • Minimising effect of variation in probability of detecting an incident case • Some use of ICISS; interest in p(admission)
Selection criteria: condition (1) • Injury surveillance • … so we first select cases in terms of injury (then external causes) • ‘Injury’ presently specified as S00-T75, T79 • Includes ‘anatomical’ trauma, burns, poisoning and ‘certain early complications of trauma’ (T79) • Similar to the STIPDA ICD-9-CM specification (except we have omitted late effects/sequelae here, since our aim is to estimate incidence of new cases in a period). • We call this ‘Community injury’, a term used to distinguish this set of cases, especially from the main other subject of ICD-10 Chapter 19, Complications of surgical/medical care, nec (T80-T88). • Can some conditions codable to other chapters of ICD reasonably be regarded as in-scope for injury? Probably so. (We’re discussing this with colleagues in Australia).
Selection criteria: condition (2) • We presently include only records in which Principal Diagnosis is in the range S00-T75, T79 • There is good reason to include these, since injury was the main reason for the episode in hospital. • What about records with at least one code in this range, but not as Principal Diagnosis? These are commonly for episodes of rehabilitation, usually following on from an acute care episode. Including them all would certainly inflate estimates of incident cases. We will review handling of this group when better person-linked files are available to us.
Selection criteria: condition (3) • Injury cases are counted whether or not the record includes an external cause code • Australian coding standards require that all cases meeting our definition of injury should have at least one external cause code. • Nearly all cases that meet other criteria do so: 99.9% in 2003-04, up from about 97% in 2001-02. • We count the rest as ‘injury cases’, though the lack of external cause codes limits analysis.
Selection criteria: condition (4) • Handling of ambiguous records • Our recent reports on hospitalised injury have focused on Community injury, but have included summary information on other cases coded to Chapter 19 of ICD-10-AM, chiefly Complications of surgical/medical care coded to T80-T88. • A small proportion of records were ambiguous, having • Principal Diagnosis = Community injury and first External cause code = Complications, or • Principal Diagnosis = Complications and first External cause code = Community injury. • We are now (2003-04 report) assigning these on the basis of Principal Diagnosis.
Selection criteria for cases due to injury and poisoning, Australia 2003–04 Includes (a) 3, and (b) 3 separations for which sex was not reported.
Community injury, Australia 1999–00 to 2003–04 Age-standardised rates
Approach to the task • recognise that our data, knowledge and methods all have substantial limitations • try to make good use of the available data • try to detect, create and make good use of opportunities to improve data, methods and our knowledge of them • don’t expect to do everything at once, but try to improve what we do with each new publication • are willing to change how we do things
Next steps • Person-based record linkage (hospital data) • Better handling of transfers, type changes and readmissions • Better understanding of cases with injury codes, but only as an additional diagnosis • Might help understanding of cases with external cause code(s) but no injury code • Linkage with deaths data • Better total measurement of serious and life-threatening injury • Greater use of ED and primary care data (where possible…) • Better understanding of admitted cases in relation to a broader segment of all injury. • Change and difference in admission fractions • External cause code validation and testing • Better understanding of the reliability of external cause coding, and ways to improve it. • Better understanding of cases with external cause code(s) but no injury code • Exploratory consideration of some diagnosis codes outside Chapter 19 for inclusion as ‘injury’ • Potential to provide a more complete measurement and description of injury