Download
1 / 37
370 likes | 484 Views
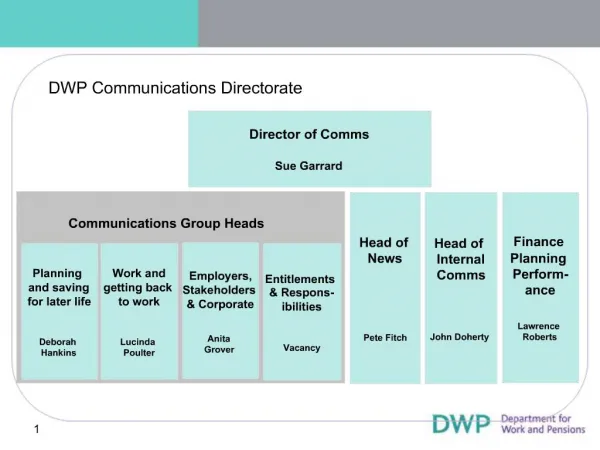
Agenda Item: 13 Paper no: CM/02/12/12. Strategic Marketing and Communications directorate Strategies overview. Contents. 2. Our Purpose.

E N D
Agenda Item: 13 Paper no: CM/02/12/12 Strategic Marketing and Communications directorate Strategies overview
Contents 2
Our Purpose ‘The purpose of the strategic marketing and communications directorate is to build CQC’s reputation as an effective and independent regulator and to create meaning from our regulatory products in order to influence health and social care policy and regulatory policy.’ • These responsibilities are discharged through the following teams: • Communications delivery • Media relations • Digital communications • Public affairs 3
Our Priorities • Although focused on particular audiences all SMC teams work to five key business priorities that bring each of the SMC strategies together. These themes underpin our actions as a team and provide a focus for our delivery. • Clarify CQC’s goals and role, build our reputation, and demonstrate that we effect change. (All strategies) • Develop a sector-led approach to help providers understand and recognise the value of our model. (Provider strategy and Digital Comms strategies) • Build understanding among people who use services of CQC’s role, the value of our public information and the importance of what people tell us in our work. (Public Comms strategy and Digital Comms strategies) • Develop a strategic approach to demonstrating effectiveness and building advocacy via media and public affairs channels. (Media strategy) • Promote staff ownership of what we do and how to improve it, by recognising how our work benefits people who use services. (Internal Comms and engagement strategies) 4
Agenda Item: 13 Paper no: CM/02/12/12 Strategy for communicating with people who use services January 2012 – April 2013
Our working assumption • We are one of a number of organisations providing valuable information about health and social care services that supports choice – the regulator’s view of whether or not providers are meeting government standards • We target our communications and resources on those who most need to know about our information and makes the information available in an accessible way • We make our findings publicly available, syndicate them through partnerships with selected third parties and tailor them to suit that partnership • We test whether our public information meets the needs of people who use services with key voluntary and statutory organisations, public focus and reference groups • We undertake pilots to identify and evaluate additional sources of user voice, build systems and processes to track soft intelligence information through our systems • We build our brand online, including our need for feedback 6 6
Where we want to be 2012 - 2013 • User communications has a clear remit • We will have defined our role in providing information for people who use services, continuing to improve it to make sure it is clear, transparent, accessible and supports our role • We will have identified new sources of valuable, structured ‘soft’ intelligence and driven improvements to the way we process them • We have improved understanding among representative groups of CQC’s role, the public benefit of what we do, and what the essential standards mean to them • We will have increased awareness of our brand online 7
Improve our public information • Continue to interpret the regulatory model into clear, transparent, accessible public information on our website, including provider profile v 2, and resolve continuing and new publication issues through a dedicated task and finish group • Improve the inspection report design and generic content and ensure staff are trained on writing clear, accessible plain English reports • Continue to improve the new website – downloadable list of up to date basic information about providers; improved search functionality; alternative formats functionality; more transparent information about services we have registered but not yet inspected; information about a service’s record of compliance; location history and deregistered services; RSS feeds • Develop a new website and public content for Healthwatch England • Highlight regular thematic reports about the state of care through fit for purpose management information • Test public facing policies, messages and products with public focus groups and public reference group; test web functionality with user testing • Post strategic review, review and refresh all corporate materials and content to provide more clarity about what we offer to the public, including clarity about role of Healthwatch England and local Healthwatch; deliver new public corporate content for mental health users 8 8
How we will deliver Testing of messages, policies and products via public focus groups and public reference groups; web functionality tested with user testing 9
Agenda Item: 13 Paper no: CM/02/12/12 Provider communications strategy review April 2012 - March 2013
Moving providers from ‘understanding’ to ‘accepting’ NHS/ASC/IH providers Dental / ambulance providers Primary medical services 14 14
How we will deliver 15 15
Agenda Item: 13 Paper no: CM/02/12/12 Digital Strategy (excluding Online Services) April 2012 - March 2013
Summary objectives for the coming year – for the public • Ensure that CQC’s work is seen much more widely. • Adapt to become a provider of syndication products • Raise awareness online of the fact that CQC needs to know about people's experience of care. • Gather more information about people's experience of care from our website & from other places around the web • Ensure that CQC’s judgments and reports are published accurately and on time – and shine a light on any parts of publication process that need to be improved • Work to make CQC a more transparent organisation 18
What we will be doing & what we willbe measured on Getting more views of our reports (on our site or syndicated versions) Syndicating CQC data to support the market in providing information for the public Adapting to become a supplier of syndicated information Making CQC more transparent Improving the end to end publication process Developing & promoting our “Please share your experience” offering Listening in to people's experience of care elsewhere Doing better in Google search results Improving our Twitter, Facebook & email engagement Delivering Provider Profile 2 Delivering the HealthWatch England website Delivering a roadmap of new website features Working internally to promote consistent design & comms standards across all digital products 19
2. Syndicating CQC data to support the market in providing information for the public • CQC will start to actively support the rapidly growing market in providing information aimed at helping the public choose the best places to get care. • We believe that the public benefit from this market and we want to ensure that CQC information is a prominent component of what people see when they are researching their care on any of these sites. • We will seed this market by making our valuable, comprehensive and accurate directory of providers available free to anyone with the condition that CQC is credited and linked through to. • This arrangement will result in the public getting better access to CQC information across the web as well as making it easier for the market to develop new ways of providing all kinds of useful information for people who are researching care. 20
2. Syndicating CQC data to support the market in providing information for the public The CQC widget – about to be piloted with providers, who will able to embed summary CQC information onto their own websites A current example of a website using CQC’s directory – and linking back to CQC’s reports http://www.goodcareguide.co.uk/provider/the-grange-care-centre-ub12qw/?referrer=search 21
6. Developing & promoting our “Please share your experience” offering • The “Please share your experience” feature has been on the CQC website since its relaunch in Oct 2011. We currently receive a comparatively small number of responses per month (about 450) which feed into CRM & the QRP. • Engaging the public to help CQC monitor the places where they receive care is vital to CQC’s overall strategy and we will continue to develop this feature and promote it in conjunction with the public comms team. Part of the promotion of this feature needs to be communicating success stories of improvement resulting from the public telling CQC what they have seen. • We also note that Ofsted are now offering a “trip advisor” feature on their website. Although we have no current plans to do similar, we will keep an open mind on this. • In the Provider Profile 2 development we will make the “Please tell us your experience” feature more prominent and look at whether the page designs should give equal emphasis to “Our reports” and “Your view”. • We will look at ways of telling people summary information about what we are receiving (that may in itself encourage other people to send information) eg – “38 people have sent us feedback on this service”. • We will work with Intelligence, Data management and NCSC to ensure that we can deal with greater volumes of public feedback. 22 22
Update on the “Please share your Experience form” The Your Experience form launched when the new website went live on 19 October 2011. In the first four months, 1,521 forms were completed, with around half of these raising urgent concerns. An update to the form went live when the R&RA and Patients Association pilots launched on 12 March. This means urgent concerns are now being sent directly to the Safeguarding team. Benefits Prominence: The ability to have your say on services you use is now one of the key messages given to visitors to our website. Easy to find: the form is at the centre of every location profile page – more than 10,000 are viewed each day. Reduction in calls: NCSC have seen a significant reduction in web queries since launch while receiving more feedback. Structured feedback: The information we receive is now tied to a location, easily passed to an inspector and suitable for QRP. 23 23
Media strategy Agenda Item: 13 Paper no: CM/02/12/12 Media StrategyApril 2012 – October 2012
Context • This Media Strategy for April – October 2012 sets out how the media team will seek to support CQC’s organisational priorities and the achievement of its objectives. It: • Assesses CQC’s current media profile, focussing on spikes of negative and positive coverage, analyses what we have learnt from these and the factors that have contributed to our current position. • Identifies the four-stage journey along which we need to move public perception, via the media, toward recognition of the benefits and impact of our regulation; and maps actions against these stages. • Outlines the programme of media activity for the next seven months. • It has interdependencies with and is aligned to other strategies (primarily the Stakeholder and Parliamentary Strategy). Big ticket’ items i.e.T5 registration have their own project-specific communication plans. 25
How have we got here? • Inherent risk • Scale and nature of our regulatory responsibilities; measured by scale and likelihood of harm, we regulate the UK’s most high-risk industry - far larger and more complex than UK aviation industry. • Acquired risk: • At the outset, CQC positioned itself as an improvement agency. We over-estimated what we could deliver – and have spent the last four years trying to climb down from this position and to sell a less palatable, more complex message to a public who understand us to be responsible for improving services. • Bringing together three legacy organisations resulted in redundancies and low staff morale, with some staff expressing their dissatisfaction publically. 26
Where do we need to be? • Growing tendency in the media to view CQC as ‘set up to fail’ – our remit is too large, our resources too stretched, our funding inadequate. • While this is preferable to a view that failures to spot poor care are due to inefficiency, it’s still precarious positioning. The truth is that even if our resources were doubled, we would still not be able to identify and prevent all poor care. • This is what we need to communicate, and which we can only do by fundamentally changing expectations of what regulation can – and should be expected to – achieve. • Changing perception takes time – and changing perception from a position of weakness takes even longer. We need be realistic about what we can achieve and by when – especially given a year ahead that includes Mid Staffs. • Until we can demonstrate that we take swift, decisive action supported by a robust evidence base, we will struggle to achieve any sustained improvement in our media profile. 27
What tools do we need to get there? • In order to tell a convincing story which describes an effective organisation, we need: • The right evidence – timely inspection reports describing consistent judgements on compliance in a way which is meaningful to the public and providers. • The right action – transparent, proportionate enforcement action that utilises the full range of our powers. • The right information – robust data and management information that allows us to speak with authority on the sectors we regulate. • The right level of influence – among key stakeholders, policy makers, opinion formers. 28
National and Regional coverage bysentiment, Jan – April 2012
What needs to change? How do we use the media to move public perception toward recognition of the benefits and impact of our regulation? Demonstrate effectiveness Clarify our role Build advocacy Drive the debate 30
Demonstrate effectivenessHow do we get there? • Use State of Care and accompanying market reports as evidence base to demonstrate scale and impact of our work, allowing us to tell a clear story on: • - numbers of inspections; • - number and location of non-compliant providers; • - key themes of non-compliance; and • - how many have gone from non-compliance to compliance / closure (ASC). • Hold press briefing to accompany every quarterly report. Establish as a key event in the health and social care calendar - most comprehensive update available on performance across the health and social care sectors and what the impact of regulation is. • Use national and regional coverage of themed inspection programmes. We know this model - unannounced inspections highlighting failings at individual providers with a national report summarising findings – resonates with public expectations of CQC. 31
Demonstrate effectivenessHow do we get there? • To build on the success of DANI 1 – and ensure that front pages translate into ‘reputation capital’ for CQC – we should: • Ensure every themed inspection programme identifies national case studies, including stories of service users, experts by experience, support from clinical experts; • Hold a press conference for every themed inspection national report; • Issue local press notices for every single piece of non-compliance found through themed inspections including all the numbers about the national programme, and to pursue these with local media – supported by rigorous follow-up by Ops; • Support themed inspections through Twitter campaign nationally and regionally; and • Where possible, identify improvement narratives - where providers have returned to compliance - as well those where further action has been necessary. 32
Clarify our roleHow do we get there? • In order to be clear about what space we don’t occupy, we need to demonstrate our effectiveness before we can clarify our role - through unambiguous messaging about the limits of regulation in a way that is not construed as ‘buck-passing’. • Use all our media work - and SoC and themed reviews in particular - as vehicles for this messaging: • Primary responsibility for providing safe and good quality care rests with providers – not with the regulator. Clear directive from DH Capability and Performance Review: • “On one key point…it is important to be clear; the responsibility to comply with essential standards of safety and quality rests squarely with the provider organisation – be it a hospital, a care home or another type of provider. CQC’s role is to inspect, to verify and to enforce when necessary.” • 2. We are not an improvement agency. While our regulation can have the effect of driving improvement, our focus is on identifying poor care and prompting action in response to this. 33
Clarify our roleHow do we get there? • Use stakeholder voices as media spokespeople to emphasise that we are not the only body with responsibility for underperformance - in particular, professional regulators, who can operate in more of an improvement space than we can. • Use BHRT 6 month review and subsequent policy piece to pose questions about how realistic radical enforcement is in relation to a maternity unit – and what other levers are available. How can the regulator influence the broader system? • Ongoing programme of media briefings: • Meetings with national health and social affairs correspondents (with repeat meetings in September to evaluate progress). • Briefings between CQC staff and key broadcast production teams (starting with Today programme.) • Trade press briefings with national clinical advisors • RCM contact programme with key regional journalists • ‘Press breakfast’ for key national correspondents to seek their views on CQC – what we do well or poorly. 34
Build AdvocacyHow do we get there? • Write to every key stakeholder with a summary of every themed inspection • Ensure stakeholder/advisory groups are engaged in themed inspections from the outset – not as an afterthought. • Flag to relevant stakeholders in advance if we are aware that a negative report/issue is due to hit the media – they are more likely to respond in a considered manner if forewarned. • Ensure that when we publish consultation responses, we are as transparent as possible about responses received - and if these have not been reflected, why not. • Use SoC and market reports to increase engagement with MPs on a constituency basis using regionally-focused data. • Communicate what we do to HSC and PAC better. 35
Drive the debateHow do we get there? • Use State of Care, accompanying market reports and national reports on thematic reviews to capitalise on our access to uniquely detailed sector/provider information in order to position CQC as an authoritative voice by: • Identifying emerging trends, risks and sector challenges - enabling us to predict, rather than just react to, service/market failure. • Using our information to help stakeholders and policy makers develop a meaningful policy response. • Including comment on our findings from key sector stakeholders reflecting on our findings, what they say about the emerging challenges for each sector – and what need to happen to effect change. • Using academic partnership/advisory group input to add additional dimension to national reports and ensuring that these move beyond identifying poor care to ‘call for action’. • Develop clear positioning for Chair and Chief Executive - define a distinct but complementary 'space' for each to occupy and from which they can promote agreed narratives externally. 36
How do we evaluate? • Track sentiment; reach; message pick-up via quarterly media analysis • Incorporate media-specific element of public perception audit into impact analysis • Engage Stakeholder Committee in qualitative testing on media perceptions of regulation • Actively building questions about media perception into Mori survey • Test with stakeholder reference group - annual survey - i.e. based on this year's coverage, which of the following statements about the CQC do you agree with? • Repeat current programme of meetings with health and social affairs correspondents in September for an informal ‘pulse check’ – do they believe we are doing a better job of explaining what we do? (key criticism currently) 37