Download
1 / 1
10 likes | 191 Views
Background.

E N D
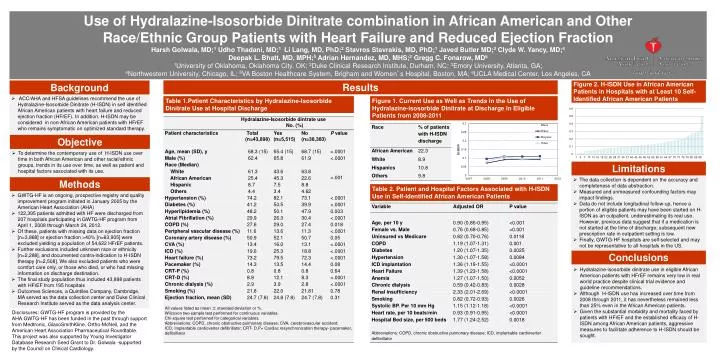
Background • ACC/AHA and HFSA guidelines recommend the use of Hydralazine-Isosorbide Dinitrate (H-ISDN) in self identified African American patients with heart failure and reduced ejection fraction (HFrEF). In addition, H-ISDN may be considered in non-African American patients with HFrEF who remains symptomatic on optimized standard therapy. Objective • To determine the contemporary use of H-ISDN use over time in both African American and other racial/ethnic groups, trends in its use over time, as well as patient and hospital factors associated with its use. Methods Use of Hydralazine-Isosorbide Dinitrate combination in African American and Other Race/Ethnic Group Patients with Heart Failure and Reduced Ejection Fraction Harsh Golwala, MD;1 Udho Thadani, MD;1 Li Lang, MD, PhD;2 Stavros Stavrakis, MD, PhD;1 Javed Butler MD;3 Clyde W. Yancy, MD;4 Deepak L. Bhatt, MD, MPH;5 Adrian Hernandez, MD, MHS;2 Gregg C. Fonarow, MD6 1University of Oklahoma, Oklahoma City, OK; 2Duke Clinical Research Institute, Durham, NC; 3Emory University, Atlanta, GA; 4Northwestern University, Chicago, IL; 5VA Boston Healthcare System, Brigham and Women’s Hospital, Boston, MA; 6UCLA Medical Center, Los Angeles, CA Results Figure 2. H-ISDN Use in African American Patients in Hospitals with at Least 10 Self-Identified African American Patients Table 1.Patient Characteristics by Hydralazine-Isosorbide Dinitrate Use at Hospital Discharge Figure 1. Current Use as Well as Trends in the Use of Hydralazine-isosorbide Dinitrate at Discharge in Eligible Patients from 2008-2011 Limitations • The data collection is dependent on the accuracy and completeness of data abstraction. • Measured and unmeasured confounding factors may impact findings. • Data do not include longitudinal follow-up, hence a portion of eligible patients may have been started on H-ISDN as an outpatient, underestimating its real use. However, previous data suggest that if a medication is not started at the time of discharge; subsequent new prescription rate in outpatient setting is low. • Finally, GWTG-HF hospitals are self-selected and may not be representative to all hospitals in the US. Table 2. Patient and Hospital Factors Associated with H-ISDN Use in Self-Identified African American Patients • GWTG-HF is an ongoing, prospective registry and quality improvement program initiated in January 2005 by the American Heart Association (AHA) • 122,395 patientsadmitted with HF were discharged from 207 hospitals participating in GWTG-HF program from April 1, 2008 through March 24, 2012. • Of these, patients with missing data on ejection fraction [n=3,868] or ejection fraction >40% [n=63,905] were excluded yielding a population of 54,622 HFrEF patients. • Further exclusions included unknown race or ethnicity [n=2,288], and documented contra-indication to H-ISDN therapy [n=2,508]. We also excluded patients who were comfort care only, or those who died, or who had missing information on discharge destination. • The final study population thus included 43,898 patients with HFrEF from 195 hospitals • Outcomes Sciences, a Quintiles Company, Cambridge, MA served as the data collection center and Duke Clinical Research Institute served as the data analysis center. Conclusions • Hydralazine-isosorbidedinitrate use in eligible African American patients with HFrEF remains very low in real world practice despite clinical trial evidence and guideline recommendations. • Although H-ISDN use has increased over time from 2008 through 2011, it has nevertheless remained less than 25% even in the African American patients. • Given the substantial morbidity and mortality faced by patients with HFrEF and the established efficacy of H-ISDN among African American patients, aggressive measures to facilitate adherence to H-ISDN should be sought. Disclosures: GWTG-HF program is provided by the AHA.GWTG-HF has been funded in the past through support from Medtronic, GlaxoSmithKline, Ortho-McNeil, and the American Heart Association Pharmaceutical Roundtable. This project was also supported by Young Investigator Database Research Seed Grant to Dr. Golwala -supported by the Council on Clinical Cardiology.